Nervous System Part 2 (Viva)
6 years ago 5576
Q.188 Name the parts of the cerebellum.
Q.189 Name the phylogenetic divisions of the cerebellum.
Q.190 Name the functional divisions of the cerebellum.
Q.191 What are the histological structures of the cerebellum?
Q.192 Name the afferent nerve fibers to the cerebellar cortex.
Q.193 Name the cerebellar nuclei.
Q.194 What are the nerve fibers of the white matter of the cerebellum?
Q.195 How are the projection fibers of the cerebellum arranged?
Projection fibers of the cerebellum are arranged in three bundles:
Q.196 What are the components of the vestibulocerebellum?
Vestibulocerebellum includes the flocculonodular lobe which is formed by nodulus of the vermis and the lateral extension on either side called flocculus.
Q.197 What are the functions of the vestibulocerebellum?
Vestibulocerebellum regulates tone, posture, and equilibrium because of its connections with the vestibular apparatus, vestibular nuclei, and spinal motor neurons.
Q.198 Name the components of spinocerebellum.
Lingula, central lobe, culmen, lobulus simplex, declive, tuber, pyramid, uvula, paraflocculi and medial portions of cerebellar hemispheres.
Q.199 What are the functions of spinocerebellum?
Q.200 What are the components of corticocerebellum?
Lateral portions of the cerebellar hemispheres.
Q.201 What are the functions of corticocerebellum?
Corticocerebellum is concerned with the integration and regulation of muscular activities because of its afferent and efferent connections with the cerebral cortex through the Cerebro-cerebello-cerebral circuit. Cerebellum also receives feedback signals from the muscles during muscular activity.
Q.202 What is Charcot’s triad?
It is a syndrome characterized by nystagmus, intention tremor, and scanning speech due to disturbances of cerebellar connection with the brainstem which generally occurs during disseminated sclerosis.
Q.203 Name the mechanisms of action of corticocerebellum.
Corticocerebellum acts by:
Q.204 What are the effects of cerebellar lesion?
Q.205 What are the disturbances in tone and posture during cerebellar lesion?
Q.206 What are the disturbances in equilibrium during cerebellar lesion?
While standing: The legs are spread to provide a broad base and the body sways from side to side with oscillation of head
While moving: Staggering, reeling, and drunken like gait is observed.
Q.207 What are the disturbances in movements during cerebellar lesion?
Q.208 What are basal ganglia?
Basal ganglia are the scattered masses of gray matter submerged in subcortical substances of the cerebral hemisphere. Basal ganglia form the part of the extrapyramidal system, which is concerned with the integration and regulation of motor activities.
Q.209 What are the primary components of basal ganglia?
Q.210 Give an account of hyperkinetic syndrome of basal ganglia.
Hyperkinetic syndrome may be due to:
Q.211 What are the parts of the corpus striatum?
Corpus striatum includes:
Q.212 What are the functions of basal ganglia?
Q.213 Name the disorders of basal ganglia.
Q.214 What is the cause of Parkinson’s disease?
Parkinson’s disease or Parkinsonism is due to the damage of basal ganglia. It is mostly because of deficiency or lack of dopamine that is secreted by dopaminergic fibers of nigrostriatal pathway.
Q.215 What are the symptoms of Parkinson’s disease?
Q.216 Name the lobes of the cerebral cortex.
Q.217 What are the functional divisions of the frontal lobe?
The frontal lobe is divided into two parts on the basis of functions:
Q.218 What are the parts of the precentral cortex or excitomotor cortex?
Q.219 What are the functions of the precentral cortex?
The primary motor area of the precentral cortex is concerned with the initiation of voluntary movements and speech. The Premotor area is responsible for movements of the tongue, lips, and larynx, which are involved in speech. The supplementary motor area is concerned with skilled movements.
Q.220 How is the localization or homunculus in the motor area designed?
Muscles of various parts of the body are represented in area 4 in an inverted way from medial to lateral surface. The lower parts of the body are represented in the medial surface and the upper parts of the body are represented in the lateral surface. The order of representation from medial to lateral surface is toe, ankle, knee, hip, trunk, shoulder, arm, elbow, wrist, hand, fingers, and face. However, the face is not represented in an inverted manner.
Q.221 What are the areas present in the prefrontal cortex or orbitofrontal cortex?
Areas: 9, 10, 11, 12, 13, 14, 23, 24, 29, and 32.
Q.222 What are the functions of the prefrontal cortex?
Q.223 What is frontal lobe syndrome? What are its important features?
The signs and symptoms, which occur due to injury or ablation of the prefrontal cortex are together called frontal lobe syndrome.
Important features:
Q.224 What do you mean by amnesia, retrograde amnesia and anterograde amnesia?
Q.225 Name the functional areas of the parietal lobe.
Q.226 What are the functions of somesthetic areas of the parietal lobe?
Somesthetic area I is responsible for the perception and integration of cutaneous and kinesthetic sensations. Area 1 is concerned with sensory perception. Areas 2 and 3 are involved in the integration of these sensations. Somesthetic area II is also concerned with the perception of sensation. Somesthetic association area is concerned with combined sensations like stereognosis.
Q.227 How is the localization or homunculus in the primary sensory area designed?
The sensory areas of the body are represented in the primary sensory area in an inverted manner. The toes are represented in the lower part of the medial surface, legs at the upper border, then from above downwards – knee, thigh, hip, trunk, upper limb, neck, and face. The representation of the face is not inverted.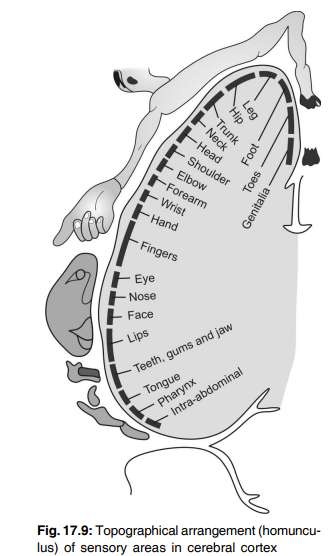
Q.228 What is the sensory-motor area?
The sensory area in the postcentral gyrus extends anteriorly into the precentral gyrus of the frontal lobe, i.e. the motor area. Similarly, the motor area is extended from the precentral gyrus posteriorly into the postcentral gyrus. So, the precentral and postcentral gyri are knit together by association neurons and are interrelated functionally. This area where both motor and sensory neurons are present is called the sensory-motor area.
Q.229 What is the function of the sensory-motor area?
The sequential movements, which are timed and programmed by corticocerebellum are stored in the sensory-motor area.
Q.230 Name the areas of the temporal lobe.
Q.231 What are the functions of the primary auditory area?
Primary auditory area is concerned with the perception and interpretation of auditory impulses. Areas 41 and 42 are concerned with the perception of auditory impulses. Wernicke’s area (along with auditopsychic area – area 22) is responsible for the interpretation of sound.
Q.232 What is temporal lobe syndrome or Kluver-Bucy syndrome?
This is the condition that occurs in animals particularly in monkeys after the bilateral ablation of the temporal lobe along with amygdaloid and uncus. It occurs in human beings during the bilateral lesion of these structures.
Q.233 What are the manifestations of temporal lobe syndrome?
Q.234 What are the areas of the visual cortex?
Q.235 What are the functions of areas of the visual cortex?
Primary visual area (17) is concerned with the perception of visual impulses. The visual association area (18) is concerned with the interpretation of visual impulses. The occipital eye field (19) is concerned with the movement of eyeballs.
Q.236 Define limbic system.
The limbic system is a group of cortical and subcortical structures, which form a limbus or ring around the hilus of the cerebral hemisphere.
Q.237 What are the structures of the limbic system?
Q.238 What is Papez circuit?
The interconnections between the various structures of the limbic system form a complex closed circuit called the Papez circuit.
It includes:
Hippocampus → mammillary bodies → thalamus → cingulate gyrus of cortex → hippocampus.
Q.239 What are the functions of the limbic system?
Q.240 Define reticular formation.
The reticular formation is a diffused mass of neurons and nerve fibers forming an ill-defined meshwork of reticulum in the central portion of the brainstem.
Q.241 Name the divisions of reticular formation.
Q.242 What are the functions of the ascending reticular activating system (ARAS)?
Q.243 What are the classical or specific sensory pathways?
Classical or specific sensory pathways are the pathways that transmit the sensory impulses from receptors to the cerebral cortex via the thalamus.
Q.244 What are the functions of descending inhibitory reticular formation?
Control of somatomotor system – it is responsible for the smoothness and accuracy of movements by regulating the muscle tone
Control of vegetative functions like cardiac function, blood pressure, respiration, gastrointestinal function, and body temperature.
Q.245 What are the functions of descending facilitatory reticular formation?
Q.246 What is decorticate preparation?
The animal in which all the connections of the cerebral cortex are cut is called decorticate preparation. The basal ganglia and brainstem are kept intact.
Q.247 What are the features of decorticate animals?
There is an extension of lower limbs and flexion of upper limbs at the elbow joint across the chest. The wrists and fingers are also flexed. When the neck is turned to one side, there is flexion of lower and upper limbs on the opposite side.
Q.248 What is decerebrate preparation?
In this, all the connections of cerebral hemispheres are removed at the level of the midbrain by sectioning between superior and inferior colliculi.
Q.249 What are the features of decerebrate preparation?
It is characterized by a state of stiffness called decerebrate rigidity resembling the effects of upper motor neuron lesion. There is an extension of all the limbs, extension of the tail, and arching of the back. This type of attitude is called opisthotonus.
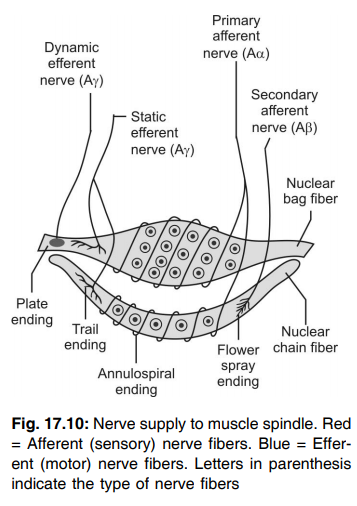
Q.250 Name the intrafusal fibers which form the muscle spindle.
Q.251 What is the unique feature of the muscle spindle?
The muscle spindle is the only receptor in the body, which is innervated both by sensory nerve fibers and motor nerve fibers.
Q.252 Brief the innervation of muscle spindle.
The following are nerve supply of muscle spindle
Sensory nerve supply:
By two types of sensory nerve ending:
Motor nerve supply:
By gamma motor neurons belonging to type A gamma fibers.
Q.253 What are the functions of the muscle spindle?
The muscle spindle gives a response to change in the length of the muscle fiber.
It has two functions:
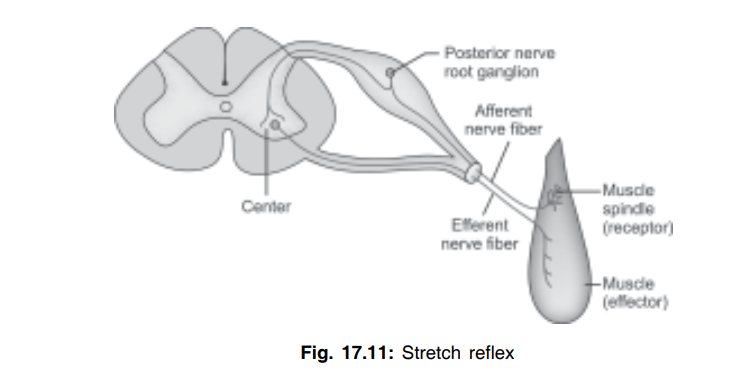
Q.254 What is stretch reflex?
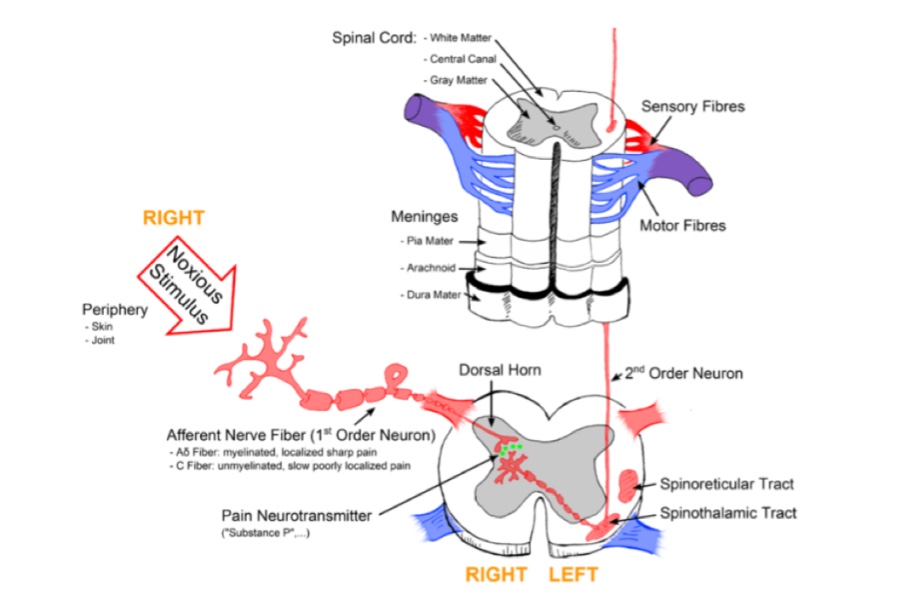
When a muscle is stretched, it contracts reflexly. This is called stretch reflex or myotatic reflex. It is a monosynaptic reflex and the quickest of all the reflexes.
Q.255 What is the Golgi tendon organ? What is its nerve supply?
It is a proprioceptor situated in the tendon of the muscle. It is supplied by sensory nerve fiber belonging to the type A beta group.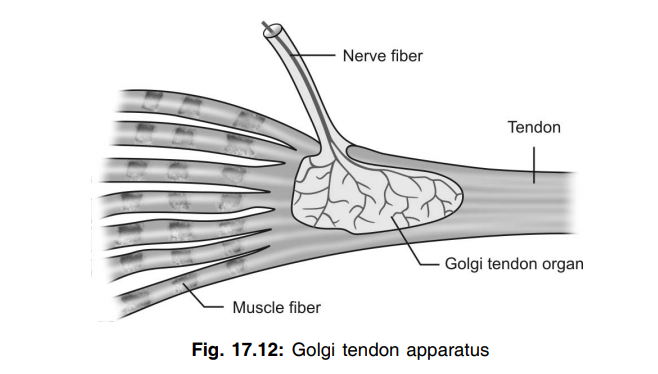
Q.256 What are the functions of the Golgi tendon organ?
Golgi tendon organ is concerned with:
Q.257 What is an inverse stretch reflex?
The relaxation of the muscle due to powerful stretch is called the inverse stretch reflex. It is the inhibition of contraction of extrafusal fibers due to excessive stretching. So, it is called autogenic inhibition.
Q.258 What do you mean α−γ linkage?
For the maintenance of muscle tone, the impulses from the γ motor neuron causes contraction of the end portion of intrafusal fibers resulting in stretching of the muscle spindle. This leads to the discharge of impulses from the primary sensory nerve endings. These impulses stimulate the α motor neurons of the spinal cord which in turn send impulses to extrafusal fibers and cause contraction of extrafusal muscle. This is known as α−γ linkage.
Q.259 What is reciprocal inhibition?
When a stretch reflex is induced, the activity of afferent fibers from the muscle spindle excites the motor neurons supplying the muscle from which the impulses come and inhibits those supplying its antagonist muscle. This phenomenon is called as reciprocal inhibition.
Q.260 Compare monosynaptic and polysynaptic reflex.
| Parameter | Monosynaptic | Polysynaptic |
| No of synapse | Only one | Many |
| Latent period | Shorter | Comparatively longer |
| Important feature | Do not have a phenomenon of after discharge | Present |
| Example | Stretch reflex | Withdrawal and superficial reflex. |
Q.261 What is lengthening reaction?
In a decerebrate animal, some resistance is offered when the arm is flexed at the elbow joint passively. This resistance is offered because of the stretch reflex developed in the triceps muscle. However, if the forearm is flexed forcefully, the resistance to flexion is abolished suddenly, leading to quick flexion of the arm. This is called lengthening reaction. And it is due to the activation of the Golgi tendon organ.
Q.262 Define posture.
Posture is defined as the subconscious adjustment of tone in different groups of muscles in accordance with every movement of the body.
Q.263 What is the significance of posture?
Posture helps to have smooth and accurate movements and also to maintain the body in equilibrium with the line of gravity.
Q.264 Name the basic phenomena of posture.
Muscle tone and stretch reflex.
Q.265 What are the types of postural reflexes?
Q.266 Name the types of static postural reflexes.
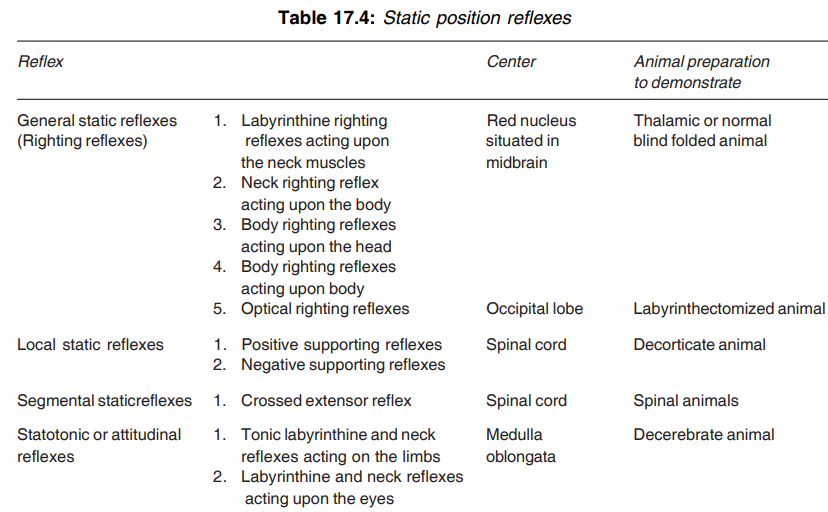
Q.267 Define general static or righting reflexes.
General static or righting reflexes are the postural reflexes, which help to maintain the upright position of the body.
Q.268 Name the righting reflexes.
Q.269 Where are the centers for righting reflexes situated?
Centers for all the righting reflexes except optic righting reflexes are in the midbrain. The center for optical righting reflexes is in the cerebral cortex.
Q.270. What is the significance of local static or supporting reflexes?
Local static or supporting reflexes support the body against gravity in different positions and also protect the limbs against hyperextension or hyperflexion.
Q.271 Name the supporting reflexes. Where is their center situated?
Q.272 Name the segmental static reflex.
The crossed extensor reflex is the segmental static reflex. (Refer Question 99 of this section for details).
Q.273 Define statotonic or attitudinal reflexes.
Statotonic or attitudinal reflexes are the postural reflexes developed according to the attitude of the body.
Q.274 What are the types of statotonic reflexes? Where is their center situated?
Q.275 What are the statokinetic reflexes?
Postural reflexes concerned with angular (rotatory) and linear (progressive) movements are known as statokinetic reflexes.
Q.276 What are the parts of the labyrinth or inner ear?
Q.277 What is vestibular apparatus? What are its parts?
The vestibular apparatus is a part of the inner ear concerned with the maintenance of posture and equilibrium. It consists of semicircular canals and otolith organs.
Q.278 What is an otolith organ?
The otolith organ is part of the vestibular apparatus. It is formed by utricle and saccule.
Q.279 Name the semicircular canals of the vestibular apparatus.
Q.280 How are the semicircular canals situated?
Anterior and posterior semicircular canals are situated vertically. The lateral semicircular canals are situated horizontally.
Q.281 What is ampulla?
The enlarged portion of each semicircular canal is known as ampulla.
Q.282 What is crista ampullaris?
Crista ampullaris is the receptor organ in the ampulla of semicircular canal.
Q.283 Name the receptor cells of crista ampullaris?
Type I and type II hair cells.
Q.284 What are stereocilia?
Stereocilia are the cilia arising from the cuticular plate in the apex of hair cells of crista ampullaris.
Q.285 What is kinocilium?
Kinocilium is the largest cilium of hair cells of crista ampullaris.
Q.286 What is macula?
The macula is the receptor organ of the otolith organ.
Q.287 How is the macula of the otolith organ situated?
The macula of the utricle is situated in a horizontal plane so that, the hair cells are in a vertical position. The macula of the saccule is situated in the vertical plane so that, the hair cells are in a horizontal position.
Q.288 Name the nerve supplying the vestibular apparatus.
Vestibular division of vestibulocochlear nerve
Q.289 What are the functions of the vestibular apparatus?
Q.290 What is the function of semicircular canals?
Semicircular canals are responsible for the maintenance of posture and equilibrium during rotatory movements or angular acceleration of the head in vertical, anteroposterior or transverse axis.
Q.291 What is the function of the otolith organ?
The otolith organ is responsible for the maintenance of posture and equilibrium during linear acceleration or progressive movements. Utricle is concerned with horizontal acceleration and saccule is concerned with vertical acceleration.
Q.292 What is nystagmus?
The characteristic to and fro movements of the eyeball, which occur during rotation in a horizontal plane is known as nystagmus.
Q.293 What are the components of nystagmus?
Slow component: At the beginning of the rotation of the head, the eyeballs rotate in the opposite direction of the head slowly
Quick component: When slow movements of eyeballs stop, the eyeballs move quickly to the new fixation point in the direction of rotation of the head.
Q.294 What are the causes of the slow and quick components of nystagmus?
The slow component of nystagmus is due to the vestibulocochlear reflex which is produced when the labyrinthine impulses reach the ocular muscles. The quick component is due to the activation of some centers in the brainstem.
Q.295 What are the effects of labyrinthectomy?
Removal of labyrinthine apparatus on both sides (bilateral) causes loss of equilibrium and loss of hearing sensation. Removal of the labyrinthine apparatus on one side (unilateral) causes less effect on postural reflexes. Some autonomic symptoms like nausea, vomiting, and diarrhea occur.
Q.296 Define electroencephalogram or EEG.
Record or graphical registration of electrical activities of the brain is known as electroencephalogram or EEG.
Q.297 What is the significance of EEG?
EEG is useful in the diagnosis of neurological disorders and sleep disorders.
Q.298 Name the waves of EEG.
Q.299 What is alpha block?
While recording EEG with closed eyes, alpha rhythm appears. When the eyes are opened, the alpha rhythm disappears and fast, irregular, and low voltage waves appear. The disappearance of alpha rhythm is known as alpha block.
Q.300 Name the physiological conditions when delta waves appear in EEG.
Delta waves are common in early childhood during waking hours. In adults, deep sleep is the only physiological condition when delta waves appear in EEG.
Q.301 Name the pathological conditions when delta waves appear in EEG.
Q.302 What are theta waves of EEG?
Theta waves are the low frequency and low voltage waves appearing in EEG in children below five years of age.
Q.303 Define sleep.
Sleep is the mental and physical relaxation either superficially or deeply with closed eyes.
Q.304 What are the important physiological changes during sleep?
Q.305 Name the types of sleep.
Characteristics of REM sleep and non-REM sleep
| Characteristics | REM sleep | Non-REM sleep |
| Rapid eye movement | Present | Absent |
| Dreams | Present | Absent |
| Muscle twitching | Present | Absent |
| Heart rate | Fluctuating | Stable |
| Blood pressure | Fluctuating | Stable |
| Respiration | Fluctuating | Stable |
| Body temperature | Fluctuating | Stable |
| Neurotransmitter | Noradrenaline | Serotonin |
Q.306 What is REM sleep?
This is a type of deep sleep during which the eyeballs move frequently and dreams may appear. This occupies 20 to 30% of the total sleeping period.
Q.307 What are the changes noticed in EEG during REM sleep?
EEG shows irregular waves (desynchronized waves) with high frequency and low amplitude.
Q.308 What is NREM sleep?
This is the type of sleep during which the eyeballs do not move. This occupies 70 to 80% of the total sleeping period.
Q.309 What are the stages of NREM sleep?
NREM sleep is divided into four stages based on EEG pattern:
Q.310 What are the changes noticed in EEG during different stages of NREM sleep?
Q.311 What is the mechanism of sleep?
Sleep occurs due to the activation of sleep-inducing centers (raphe nucleus and locus ceruleus) and inhibition of the ascending reticular activating system (ARAS).
Q.312 What are the neurotransmitters causing sleep?
Serotonin secreted by nerve fibers from the raphe nucleus of pons – induces non-REM sleep. Noradrenaline secreted by nerve fibers from locus cereleus – induces REM sleep.
Q.313 Define epilepsy.
Epilepsy is the brain disorder characterized by convulsive seizure or loss of consciousness or both.
Q.314 What is the cause for epilepsy?
Epilepsy is due to excessive discharge of impulses from some parts of the brain, particularly the cerebral cortex.
Q.315 What are convulsive seizures?
Uncontrolled involuntary muscular contractions are called convulsive seizures.
Q.316 What are the types of epilepsy?
Q.317 Name the types of generalized epilepsy.
Q.318 Define learning.
Learning is defined as a process by which new information is acquired.
Q.319 Name the types of learning.
Q.320 What is habituation?
Habituation means getting used to something to which a person is constantly exposed. When a person is exposed to a stimulus repeatedly he starts ignoring the stimulus slowly.
Q.321 What is sensitization?
When a stimulus is applied repeatedly, habituation occurs. But if the same stimulus is combined with another type of stimulus, which may be pleasant or unpleasant, the person becomes more sensitive to the original stimulus. It is called the amplification of response or sensitization.
Q.322 Define memory.
Memory is defined as the ability to recall past experiences. It is also defined as the retention of learned materials.
Q.323 Classify memory on a physiological basis.
Q.324 Define short-term and long-term memories.
Short-term memory is the recalling of events of hours or days. Long-term memory is the recalling of events of weeks, months or years.
Q.325 What is the basic mechanism of short-term memory?
The basic mechanism of short-term memory is the development of new neural circuits by the formation of new synapses.
Q.326 What is the basic mechanism of longterm memory?
The basic mechanism of long-term memory is the reinforcement of newly formed neuronal circuits by using it often leading to consolidation and encoding of memory in different areas of the brain.
Q.327 Name the sites of encoding of memory.
Hippocampus, Papez circuit, frontal areas, and parietal areas.
Q.328 What is memory engram or memory tracing?
It is the process by which the memory is facilitated and stored in the brain by means of structural and biochemical changes.
Q.329 What is consolidation of memory?
It is the process by which a short-term memory is crystallized into a long-term memory.
Q.330 Name the drugs, which facilitate memory.
Caffeine, physostigmine, amphetamine, nicotine, strychnine, and metrazol.
Q.331 What is amnesia?
Loss of memory is known as amnesia.
Q.332 What is dementia?
Progressive deterioration of intellect, emotional control, social behavior, and motivation associated with loss of memory is known as dementia.
Q.333 What is Alzheimer’s disease?
It is a progressive neurodegenerative disease due to degeneration, loss of function, and death of neurons in many parts of the brain particularly the cerebral cortex. Dementia is a common feature of this disease.
Q.334 Define conditioned reflex.
Conditioned reflex is a reflex response acquired or learnt by experience.
Q.335 Classify the conditioned reflexes.
Q.336 How are the properties of classical conditioned reflexes demonstrated?
By the classical salivary secretion experiments devised by Ivan Pavlov.
Q.337 Classify the classical conditioned reflexes.
Q.338 What is the significance of instrumental conditioned reflexes?
Instrumental conditioned reflexes play an important role in the development of behavior patterns in an individual particularly during the learning process in childhood.
Q.339 What is the physiological basis of conditioned reflexes?
Learning and memory form the physiological basis of conditioned reflexes.
Q.340 Define speech.
Speech is the expression of thought by the production of articulate sound, bearing a definite meaning.
Q.341 What is the mechanism of speech?
The mechanism of speech is by the coordinated activities of the central speech apparatus and peripheral speech apparatus. The central speech apparatus consists of higher centers, i.e. the cortical and subcortical centers. Peripheral speech apparatus includes the larynx or soundbox, pharynx, mouth, nasal cavities, tongue, and lips. All the structures of the peripheral speech apparatus work in coordination with the respiratory system.
Q.342 What are the cortical areas concerned with speech?
Motor areas:
– Broca’s area (area 44) or speech center or motor speech area – it controls the movements of vocalization
– Upper frontal area – it controls the coordinated movements concerned with writing.
Sensory areas:
– Auditopsychic area – it is concerned with memories of the spoken words
– Visuopsychic area – it is concerned with the storage of memories of visual symbols.
Q.343 What is Wernicke’s area, Dejerine area, and sensory speech center?
Q.344 What are the motor speech areas?
It includes Broca’s area (area 44) and Exner’s area (motor writing center). Broca’s area is located in the inferior frontal gyrus in the region of the anterior and ascending rami of the lateral sulcus in the dominant hemisphere whereas Exner’s area is located in the middle frontal gyrus in the dominant hemisphere.
Q.345 Define aphasia? What is its cause?
Aphasia is defined as a loss or impairment of speech due to brain damage. It is due to damage to speech centers.
Q.346 Name the types of aphasia.
Q.347 What is dysarthria or anarthria? What is it due to?
Difficulty or inability to speak is known as anarthria or dysarthria. It is due to the paralysis or ataxia (lack of coordination) of muscles involved in speech.
Q.348 What is pure word deafness?
It is a failure to recognize spoken speech with no other defect of speech or intelligence.
Q.349 What is cerebrospinal fluid or CSF?
The fluid present in the central canal of the spinal cord, subarachnoid space, and cerebral ventricles is known as cerebrospinal fluid or CSF. It is a part of ECF.
Q.350 Which is the site of the formation of CSF?
CSF is formed by the choroid plexus, which is situated in the ventricles of cerebral hemispheres. A major portion of CSF is formed in lateral ventricles.
Q.351 What is the mechanism of formation of CSF?
CSF is formed by the process of secretion by the choroid plexus. It involves active transport with expenditure of energy.
Q.352 What are the properties of CSF?
Volume : 150 ml
Rate of formation : 0.3 ml/minute
Specific gravity : 1.005
Reaction: Alkaline.
Q.353 What is normal glucose level in CSF?
50-70 mg%
Q.354 What is the normal cerebral blood flow?
750 ml/min.
Q.355 What is the composition of CSF?
CSF consists of 99.13% of water and 0.87% of solids. Solids:
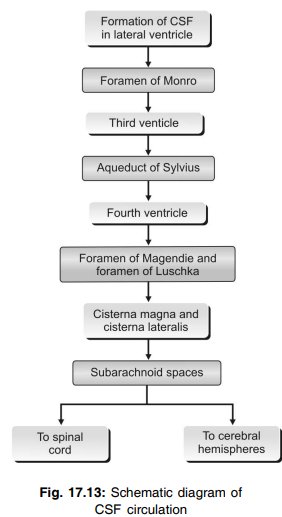
Q.356 Describe the circulation of CSF briefly.
A major quantity of CSF is formed in lateral ventricles and flows to the third ventricle through the foramen of Monro. From here, it passes to the fourth ventricle through aqueductus Sylvius. From the fourth ventricle, CSF enters cisterna magna and cisterna lateralis through the foramen of Magendie (central opening) and foramen of Luschka (lateral opening). A portion of cisternal fluid circulates through the spinal subarachnoid space. A larger part of fluid passes upwards over the brainstem through the surface of the cerebral hemispheres.
Q.357 How is CSF absorbed?
CSF is mostly absorbed by the arachnoid villi into dural sinuses and spinal veins. A small amount is absorbed along the perineural spaces into cervical lymphatics and into perivascular spaces.
Q.358 What is the mechanism of absorption of CSF?
CSF is absorbed by means of filtration due to the gradient between hydrostatic pressure in subarachnoid space and the pressure exerted by blood in the dural sinus.
Q.359 What is the normal pressure exerted by CSF?
In lateral recumbent position: 10 to 18 cm H2O.
In sitting posture: About 30 cm H2O.
Q.360 What are the functions of CSF?
Q.361 What is contrecoup injury?
When the head receives a severe blow, the brain moves forcefully and hits against the skull bone at a point opposite where the blow was applied. This leads to damage of brain tissues. This is called a contrecoup injury.
Q.362 How is CSF collected?
CSF is mostly collected by lumbar puncture by passing a needle into the subarachnoid space between 3rd and 4th lumbar spines. It is also collected by cisternal puncture by passing a needle into cisterna magna between the occipital bone and atlas.
Q.363 What is hydrocephalus? What are its effects?
Abnormal accumulation of CSF in the skull associated with enlargement of the head is called hydrocephalus. It causes atrophy of brain tissues, mental weakness, and convulsions.
Q.364 What is the blood-brain barrier?
The barrier for the passage of certain substances from blood into brain tissues is known as the blood-brain barrier.
Q.365 How is the blood-brain barrier developed?
The blood-brain barrier is developed by the formation of tight junctions between the endothelial cells of capillaries and the development of foot processes of astrocytes (neuroglia) around the capillaries.
Q.366 Name some substances, which can pass through the blood-brain barrier.
Oxygen, carbon dioxide, water, glucose, amino acids, electrolytes, and some drugs like sulfonamides, tetracycline, and many lipid-soluble substances.
Q.367 Name some substances, which cannot pass through the blood-brain barrier.
Catecholamines, penicillin, and bile pigments.
Q.368 What are the functions of the blood-brain barrier?
Q.369 What is the blood-cerebrospinal fluid barrier?
The barrier between the blood and cerebrospinal fluid existing in choroid plexus is called blood-cerebrospinal barrier fluid. It allows the movements of all the substances, which are allowed by the blood-brain barrier.
Q.370 What is the autonomic nervous system (ANS)?
ANS is the part of the peripheral nervous system that is concerned with the regulation of visceral or vegetative function of the body. It is also called a vegetative or involuntary nervous system.
Q.371 What are the divisions of ANS?
Q.372 Name the ganglia present in the sympathetic division of ANS.
Q.373 Name the nerves, which constitute the parasympathetic division of ANS.
Q.374. What are the functions of ANS?
ANS is concerned with the regulation of vegetative functions in the body, which are beyond voluntary control. By regulating various vegetative functions, ANS plays an important role in homeostasis.
Q.375 What are the neurotransmitters secreted by sympathetic fibers?
Preganglionic sympathetic fibers: Acetylcholine.
Postganglionic sympathetic adrenergic fibers: Noradrenaline.
Postganglionic sympathetic cholinergic fibers: Acetylcholine.
Q.376. Name the structures innervated by sympathetic cholinergic nerve fibers.
Blood vessels to:
• Heart
• Skeletal muscles
• Sweat glands.
Q.377 What is the neurotransmitter secreted by parasympathetic fibers?
Both preganglionic and postganglionic fibers of parasympathetic nerves secrete acetylcholine.
Q.378 What are sympathomimetic drugs? Give examples.
Drugs, which produce the effects similar to the effects of stimulation of sympathetic nerves are called sympathomimetic drugs. Examples are phenylephrine, isoproterenol, albuterol, ephedrine, tyramine, and amphetamine.
Q.379 What are sympathetic blockers? Give examples.
The drugs, which prevent the actions of sympathetic neurotransmitters are known as sympathetic blockers. Examples are reserpine, guanethidine, benzamide, phentolamine, metoprolol, and hexamethonium
Q.380 What are parasympathomimetic drugs? Give examples.
Drugs, which produce the effects similar to the effects of stimulation of parasympathetic nerves are called parasympathomimetic drugs. Examples are pylocarpine, methacholine, neostigmine, and physostigmine.
Q.381 What are parasympathetic blockers? Give examples.
Drugs, which prevent the actions of parasympathetic nerve fibers are called parasympathetic blockers. Examples are homatropine and scopolamine.
Q.382 What are ganglionic blockers? Give examples.
Drugs, which prevent the transmission of impulses from preganglionic neurons to postganglionic neurons are called ganglionic blockers. Examples are tetraethyl ammonium, hexamethonium, and pentolinium.
Also read: Nervous System Part 1 (Viva)
Comments (0)