Nervous System Part 1 (Viva)
6 years ago 14127
Q.1 What are the divisions of the nervous system?
Central nervous system (CNS) includes the brain and spinal cord.
Peripheral nervous system (PNS) that includes:
– Somatic nervous system that is concerned with movements
– Autonomic nervous system (ANS) that is concerned with visceral functions
Q.2 What are the parts of the brain?
Q.3 What are the parts of the brainstem?
Q.4 Define neuron or nerve cell.
Neuron or nerve cell is defined as the structural and functional unit of the nervous system.
Q.5 Classify the neurons.
Neurons are classified by three different methods:
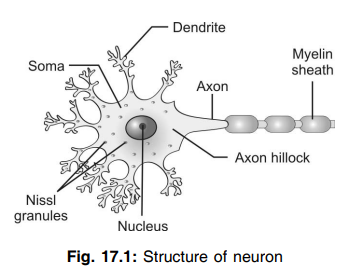
Q.6 Name the parts of a neuron.
The parts of a neuron are:
Q.7 What are the important structures present in the nerve cell body of the neuron?
Nucleus, Nissl bodies, neurofibrils, mitochondria, and Golgi apparatus.
Q.8 What are Nissl bodies? What is their function?
Nissl bodies are the small granules present throughout the soma of neuron and dendrites but not in axon hillock and axon. These bodies are responsible for the tigroid or spotted appearance of soma. Nissl bodies contain ribosomes and are concerned with the synthesis of proteins in the neuron.
Q.9 What are the processes of neuron?
Q.10 Mention the number of axon and dendrite in each neuron.
Each neuron has only one axon. The dendrite may be absent or present. If present, it may be one or many in number.
Q.11 What is an axis cylinder?
The axoplasm and the axolemma that covers the axon are together called the axis cylinder.
Q.12 What is myelin sheath?
Myelin sheath is a thick tubular sheath covering the axis cylinder.
Q.13 What is the node of Ranvier? And what is internode?
Myelin sheath is not continuous around the axon and it is absent at regular intervals. The area where the myelin sheath is absent is known as a node of Ranvier. The segment of axon between the two nodes is called the internode.
Q.14 What are the functions of myelin sheath?
Q.15 What is myelinogenesis?
The formation of the myelin sheath is called myelinogenesis.
Q.16 What are the Schwann cells? What is their function?
Schwann cells are a type of cells present in neurilemma close to axolemma. These cells are responsible for the development of the myelin sheath.
Q.17 What is neurilemma? What is its function?
Neurilemma (neurilemmal sheath or Schwann sheath) is the thin membrane that forms the outermost covering of the nerve fibers. It contains Schwann cells and so it is essential for myelinogenesis.
Q.18 Classify the nerve fibers.
Nerve fibers are classified by six different methods:
| Depending upon the structure: – Myelinated nerve fibers – Nonmyelinated nerve fibers. |
| Depending upon distribution: – Somatic nerve fibers – Autonomic nerve fibers. |
| Depending upon source of origin: – Cranial nerve fibers – Spinal nerve fibers. |
| Depending upon the functions: – Motor nerve fibers – Sensory nerve fibers. |
| Depending upon neurotransmitter secreted by them: – Adrenergic nerve fibers – Cholinergic nerve fibers. |
| Depending upon the diameter and rate of conduction of impulse: – Type A fibers – Type B fibers – Type C fibers. |
| Type A fibers are again divided into A alpha, A-beta, A gamma, and A-delta nerve fibers. |
Q.19 Name the nerve fibers conducting the impulse with maximum and minimum velocity.
Type A alpha nerve fibers conduct the impulse with maximum velocity (70 to 120 meters/second).
Type C fibers conduct the impulse with minimum velocity (0.5 to 2 meters/second).
Q.20 Distinguish between Aδ and C fibers.
| Aδ Fiber | C fibers |
| Small myelinated, 2-5 µm diameter, 12-30 mm/sec. conduction velocity | Nonmyelinated, 0.4-1.2 µm diameter with conduction velocity 0.5-2 mm/sec |
| Less in number | Relatively more |
| Conduct impulse only to noxious stimulus. | In response to thermal and mechanical stimulus |
| Sensitive to electrical stimulus. | Less sensitivity |
| Most sensitive to pressure | Most sensitive to local anesthetics and chemical factors. |
Q.21 Name the properties of nerve fibers.
Q.22 What are the two types of potentials noticed in nerve fibers?
Action potential (nerve impulse) – produced when the nerve is stimulated with adequate strength of stimulus (threshold or minimal stimulus). It is propagated and nongraded.
Electrotonic potential or local response – is produced when the strength of the stimulus is not adequate (subthreshold or sub minimal stimulus). It is non-propagated and graded.
Q.23 How much is the resting membrane potential in a nerve fiber?
About – 70 mV
Q.24 Differentiate between EPSP and AP.
| EPSP | AP |
| Stimulus intensity to generate EPSP has no threshold | Has threshold level |
| Does not obey all or none law | Obeys all or none law |
| Absence of refractory period | Present |
| Summation can occur | Never possible |
| Non-propagatory | Propagatory |
Q.25 What are the properties of generator potential?
The properties of GP are:
Q.26 What do you mean by spatial and temporal summation?
Simultaneous stimulation of two afferent nerves by a stimulus of subthreshold intensity can evoke an action potential in the motor neurons. This property is known as spatial summation.
Whereas if sub-minimal stimuli are repeated at short intervals in a single nerve, reflex action can also be evoked which is known as temporal summation.
Q.27 What is the fractionation phenomenon?
Direct stimulation of motor nerve results in more response than reflex response or in other words the tension developed reflexly is always a fraction of the response that is produced by direct motor nerve stimulation. This is known as fractionation phenomenon.
Q.28 What is afterdischarge?
Continuation of discharge of impulses from motor neurons even after withdrawal of stimulation from the sensory side is called as afterdischarge.
Q.29 What do you mean by law of forward conduction?
Synapse permits the conduction of impulse from presynaptic to postsynaptic neurons only, i.e. unidirectionally. This property is known as the law of forward conduction.
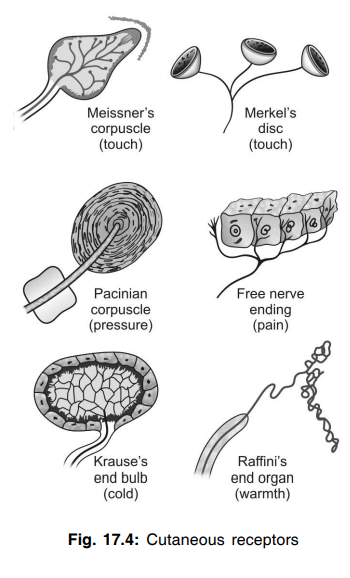
Q.30 Name the receptors responsible for following sensations—touch, pressure, hot, cold, and pain.
Q.31 Name the properties of action potential.
Q.32 What is saltatory conduction?
In a myelinated nerve fiber, the action potential (nerve impulse) jumps from one node of Ranvier to another node of Ranvier, making the velocity of conduction faster. This type of conduction in a myelinated nerve fiber is called saltatory conduction.
Q.33 Explain the mechanism of saltatory conduction briefly.
Myelin sheath is not permeable to ions. So during the conduction of action potential, the entry of sodium ions from extracellular fluid into nerve fiber occurs only at the node of Ranvier, where the myelin sheath is absent. This causes depolarization only in successive node and not in the internode. So, the action potential jumps from one node to another. Hence, it is called saltatory conduction (saltare = jumping).
Q.34Why is the nerve fiber not fatigued?
Nerve fiber is not fatigued because it can conduct only one action potential at a time. At that time it is completely refractory and cannot conduct another action potential.
Q.35 What are the changes, which take place in the nerve cell body during the degeneration of nerve fiber?
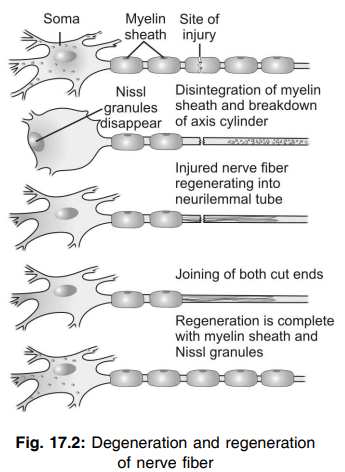
Q.36 What is Wallerian degeneration?
Degenerative change in the distal cut end of the nerve fiber is called Wallerian degeneration.
Q.37 Explain the changes during Wallerian degeneration briefly.
Q.38 What is retrograde degeneration?
The degenerative change that occurs at the proximal cut end of the nerve fiber is called retrograde degeneration.
Q.39 What is transneuronal degeneration?
If an afferent nerve fiber is cut, the degeneration occurs in the neuron with which the afferent nerve fiber synapses. This is called transneuronal degeneration.
Q.40 What are the criteria for the regeneration of nerve fiber?
Q.41 Why regeneration does not occur in the central nervous system?
Neurilemma is necessary for regeneration. But neurilemma is absent in the central nervous system, so regeneration can not take place.
Q.42 Define neuroglial cell, neuroglia or glia.
Neuroglial cell, neuroglia or glia is the supporting cell of the nervous system.
Q.43 Classify neuroglial cells.
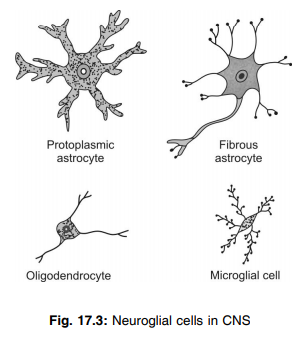
Q.44 What are the functions of neuroglia?
Astrocytes:
Microglia:
Oligodendrocytes:
Schwann cells:
Satellite cells:
Q.45 Define receptor.
The receptor is an afferent nerve terminal, which receives the stimulus. It is defined as the biological transducer that converts various forms of energy, i.e. stimulus into action potential in nerve fiber.
46. Classify receptors.
Q.47 What are the cutaneous receptors or mechanical receptors?
Receptors situated in the skin are called cutaneous receptors. The different cutaneous receptors
Q.48 What are chemoreceptors, which belong to the group of exteroceptors?
Receptors giving responses to chemical stimuli are known as chemoreceptors. The chemoreceptors, which belong to the group of exteroceptors are taste receptors in taste buds and olfactory receptors for smell in the nose.
Q.49 What are telereceptors?
The receptors, which give response to stimuli arising away from the body are called telereceptors.
Telereceptors are:
Q.50 What are visceroreceptors?
Receptors situated in the viscera are called visceroreceptors. Stretch receptors, baroreceptors, chemoreceptors, and osmoreceptors are the visceroreceptors. Visceroreceptors are situated in the heart, blood vessels, lungs, gastrointestinal tract, urinary bladder, and brain.
Q.51 Define and classify the proprioceptors.
Proprioceptors are the receptors, which give response to change in the position of different parts of the body.
Proprioceptors are of two types:
Q.52 Enumerate the properties of receptors.
Q.53 What is Doctrine of specific nerve energies or specificity of response?
Each receptor gives a response to a particular type of stimulus. For example, the pain receptors are stimulated by pain stimuli. This property of the receptor is called the Doctrine of specific nerve energies or specificity of response.
Q.54 What is adaptation?
When a receptor is continuously stimulated with the same strength of stimulus, after some time receptor stops sending impulses through afferent nerve. This property is called adaptation.
Q.55 How receptors are classified based on adaptation? Give examples.
On the basis of adaptation, receptors are classified into two types:
Q.56 What is receptor potential?
When a receptor is stimulated, a non-propagated depolarization occurs. This is called receptor potential or generator potential.
Q.57 Enumerate the properties of receptor potential.
Q.58 What is synapse?
The junction between two neurons is called a synapse. It is only a physiological continuity between two nerve cells and not the anatomical continuation.
Q.59 How is synapse classified?
Synapse is classified by two methods:
Anatomical classification:
Synapse is divided into three types depending upon the axon ending:
– Axosomatic synapse
– Axodendritic synapse
– Axoaxonic synapse.
Functional classification:
Synapse is divided into two types depending upon the transmission of impulses:
– Electrical synapse
– Chemical synapse.
Q.60 Explain the structure of axosomatic synapse briefly.
Axon of presynaptic neuron divides into many presynaptic terminals. This has a covering membrane called the presynaptic membrane. The presynaptic terminal contains mitochondria and the synaptic vesicles. Synaptic vesicles contain neurotransmitter substances. The membrane of the postsynaptic neuron is called the postsynaptic membrane. It contains receptor proteins. The space between the presynaptic and postsynaptic membrane is called the synaptic cleft. The basal lamina of the synaptic cleft contains cholinesterase.
Q.61 What is the function of the synapse?
The main function of the synapse is to transmit the impulses, i.e. action potential from one neuron to another. However, some of the synapses inhibit the transmission of impulses. Thus, synapses are of two types:
• Excitatory synapse that transmits the impulses – excitatory function
• Inhibitory synapse that inhibits the transmission of impulses – inhibitory function.
Q.62 Distinguish between electrical and chemical synapses.
| Chemical | Electrical |
| Impulse is transmitted from preto postsynaptic site through the release of neurotransmitter i.e chemical mediators | Impulse is transmitted through gap junction |
| Most of the synapses are chemical type | Present only in specific synaptic junction of brain |
| Presence of synaptic cleft | Cleft is replaced by low resistance bridges |
| Synaptic delay is present | Absent |
| Sensitive to O2 lack | Insensitive to O2 lack. |
Q.63.Explain the synaptic transmission briefly.
When an action potential reaches the presynaptic axon terminal, voltage-gated calcium channels at the presynaptic membrane open, and calcium ions enter the terminal. This causes the release of acetylcholine from synaptic vesicles. Acetylcholine passes through the presynaptic membrane and synaptic cleft and binds with receptor protein present on the postsynaptic membrane. The acetylcholine receptor complex opens ligand-gated sodium channels so that, sodium ions enter the synapse, i.e. soma. This produces excitatory postsynaptic potential (EPSP), which in turn causes the development of action potential in the initial segment of the axon of postsynaptic neurons.
Q.64 What is excitatory postsynaptic potential (EPSP)?
When an action potential reaches the presynaptic axon terminal, it causes the development of a non-propagated electrical potential in the soma of postsynaptic neurons through acetylcholine. This potential in the postsynaptic neuron is known as excitatory postsynaptic potential (EPSP).
Q.65 What are the properties of EPSP?
Q.66 What is the significance of EPSP?
EPSP causes the development of action potential in the initial segment of the axon of the postsynaptic neurons. Actually, EPSP opens sodium channels in the initial segment of axon so that sodium ions enter the axon from ECF resulting in the development of action potential.
Q.67 Name the types of synaptic inhibition.
Q.68 What is postsynaptic inhibition?
The failure of the production of the action potential in the postsynaptic membrane because of the release of an inhibitory neurotransmitter from the presynaptic terminal is called postsynaptic inhibition.
Q.69 What is postsynaptic inhibitory potential (IPSP)?
The inhibitory neurotransmitter released from the presynaptic axon terminal causes the opening of potassium channels. This results in the efflux of potassium ions from the soma of postsynaptic neurons and the development of hyperpolarization. This type of hyperpolarization is called postsynaptic inhibitory potential (IPSP).
Q.70 What is presynaptic inhibition?
In some synapses, the action potential reaching the presynaptic axon terminal fails to release neurotransmitters from the synaptic vesicles. So, the transmission of impulse is inhibited. This is called presynaptic or direct inhibition.
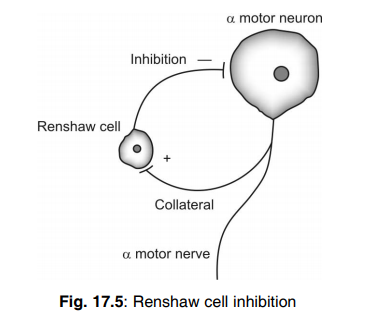
Q.71 What is Renshaw cell inhibition?
This occurs in the spinal cord. Renshaw cell is a type of motor neuron situated near the alpha motor neurons in the anterior gray horn. When alpha motor neuron of the spinal cord sends motor impulses via anterior nerve root fibers, some of the impulses reach the Renshaw cell by passing through collateral fibers. Renshaw cell in turn sends inhibitory impulses to alpha motor neurons so that, the discharge from motor neurons is reduced.
Q.72 What is the significance of synaptic inhibition?
Synaptic inhibition offers restriction over the neurons and muscles so that the excess stimuli are inhibited and the various movements are performed properly and accurately.
Q.73 Name the properties of synapse.
Q.74 What is Bell-Magendie law?
The impulses are transmitted only in one direction in the synapse, i.e. from presynaptic neurons to postsynaptic neurons. This is called Bell-Magendie law.
Q.75 What is synaptic delay? And, what is its cause?
The delay in the transmission of impulses through synapse is known as the synaptic delay.
It is due to the time taken for:
Q.76 What is the cause of fatigue in synapse?
Fatigue at synapse is due to the exhaustion of neurotransmitters.
Q.77 What is summation?
When a single presynaptic terminal is stimulated repeatedly or when many numbers of presynaptic terminals are stimulated simultaneously, there is a fusion of effects in postsynaptic neurons. This is called summation.
Q.78 What is Weber Fechner law?
The frequency of action potential in a sensory nerve is directly proportional to the magnitude of generator potential which in turn is directly proportional to the intensity of stimulus. This relationship between the intensity of stimulus, the magnitude of GP, and the frequency of AP in the afferent nerve is known as Weber Fechner law.
Q.79 What is Muller’s doctrine of specific nerve energy?
Sensation produced by impulses generated in a receptor depends on the specific part of the brain, i.e. the specific pathways for specific sensation are separated from the nerve organs to the cerebral cortex. This is known as Muller’s law.
Q.80 What do you mean by law of projection? What is a phantom limb?
No matter where a particular sensory pathways are stimulated along its course to the cortex, the conscious sensation produced is referred to as the location of the receptor. This principle is called as law of projection. A limb that has been lost by accident or amputation, the patient usually experiences intolerable pain and proprioceptive sensations in the absent limb and is called a phantom limb. Chemical and electrical synapses Chemical Electrical
Q.81 What do you mean by the law of intensity discrimination?
The brain interprets different intensities of sensations by varying the frequency of AP generated by receptor and/or by varying the number of receptors activated or both. This is known as the law of intensity discrimination.
Q.82 Name some excitatory neurotransmitter substances.
Acetylcholine, noradrenaline and histamine.
Q.83 Name some inhibitory neurotransmitter substances.
Gamma-aminobutyric acid (GABA), glycine, dopamine, and serotonin.
Q.84 Define reflex activity.
Response to a peripheral nerve stimulation that occurs without consciousness is known as reflex activity.
Q.85 What is reflex arc? Enumerate its components (parts).
The anatomical neural pathway for a reflex action is called reflex arc.
It has five components:
Q.86 What are the methods of classification of reflexes?
Reflexes are classified by five different methods:
Q.87 Classify the reflexes depending upon whether inborn or acquired.
Unconditioned reflexes which are present at the time of birth. These reflexes do not require previous learning or training or conditioning but contact of a substance with the receptor is essential. The best example is the secretion of saliva when an object is kept in the mouth
Conditioned reflexes which are acquired after birth. These reflexes require previous learning or training or conditioning and contact of a substance with receptor is not necessary. The example is the secretion of saliva by the sight, smell, thought, or hearing of a known edible substance.
Q.88 Classify the reflexes depending upon the situation of the center.
Q.89 Classify the reflexes depending upon the purpose or functional significance.
Q.90 Classify the reflexes depending upon the number of synapses.
Q.91 Classify the reflexes depending upon clinical basis.
Q.92 Enumerate the properties of reflexes.
Q.93 What are the types of summation in reflex activity?
Spatial summation: When two afferent nerve fibers supplying a skeletal muscle are stimulated separately with subliminal stimulus, there is no response. But, if both nerve fibers are stimulated together with the same strength of stimulus, the muscle contracts. This is called spatial summation.
Temporal summation: When one nerve is stimulated repeatedly with subliminal stimuli, these stimuli are summed up and cause contraction of the muscle. This is called temporal summation.
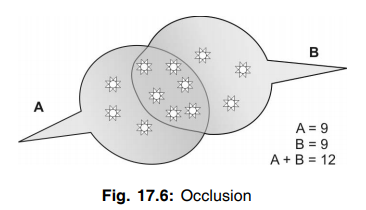
94.What is occlusion?
In a muscle which is innervated by two motor nerves called A and B, when both nerves are stimulated simultaneously, the tension developed by the muscle is less than the sum of the tension developed when each nerve is stimulated separately. This type of response is called occlusion.
For example, if nerve A is stimulated alone, the arbitrary unit of tension developed is 9. If nerve B is stimulated the tension developed is 9 units. So, the sum of tension developed when nerves A and B are separately stimulated = 9 + 9 = 18 units. But when, both A and B are stimulated together, the tension produced is (A+B) = 12 units only. This phenomenon is called occlusion and it is due to the overlapping of the nerve fibers during the distribution.
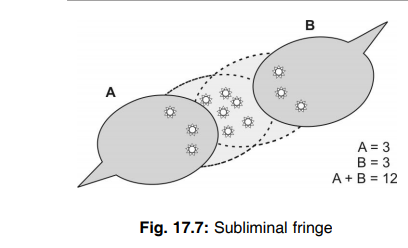
Q.95 What is sub-liminal fringe?
In some reflexes which involve the muscle with two nerve fibers called A and B, the tension developed by simultaneous stimulation of two nerve is greater than the sum of tension produced by the stimulation of these nerves separately. For example, if nerve A or B is stimulated alone, the arbitrary unit of tension developed by muscle = 3 units. So, the sum of tension developed if nerves A and B are stimulated separately is 3+3 = 6 units. But, when both the nerves are stimulated together, the tension developed = (A +B) = 12 units. So, the tension here is greater than the sum of tension produced if A and B are separately stimulated. This phenomenon is called subliminal fringe and it is due to the effect of spatial summation.
Q.96 What is recruitment?
When an excitatory nerve is stimulated with stimuli of constant strength for a long time, there is a progressive increase in the number of motor neurons activated. This phenomenon is called recruitment. It is similar to the effect of temporal summation.
Q.97 What is after discharge?
If a reflex action is elicited continuously for some time, and then the stimulation is stopped, the reflex activity i.e., contraction may continue for some time even after the stoppage of stimulus. This is called after discharge. The center discharges impulses even after stoppage of stimulus. This is because of internuncial neurons, which continue to transmit afferent impulses even after the stoppage of stimulus.
Q.98 Which is the first seat of fatigue in reflex arc?
The center or the synapse of the reflex arc is the first seat of fatigue.
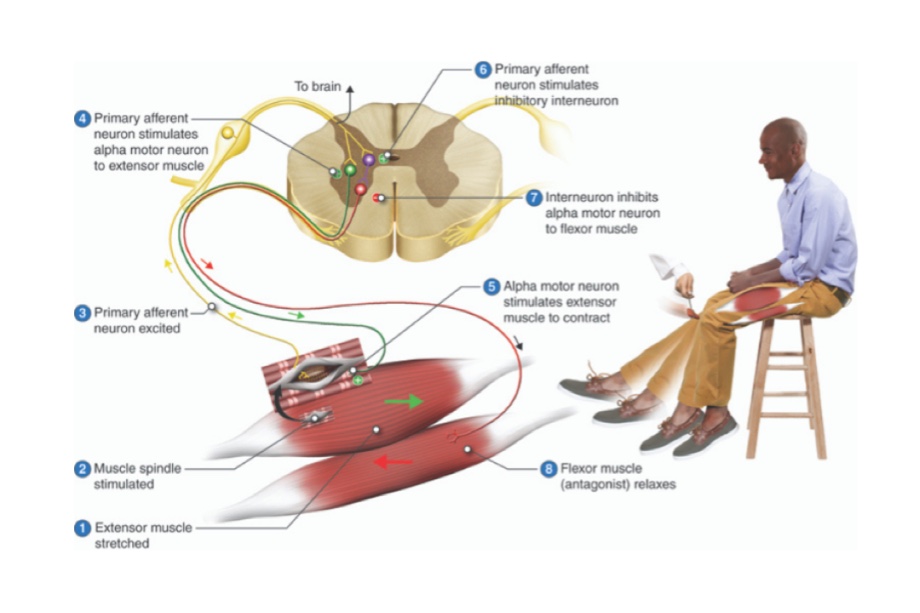
Q.99 What is crossed extensor reflex?
When a flexor reflex is elicited in one limb, the flexor muscles of that limb are stimulated and the extensor muscles are inhibited. But on the opposite limb, the flexors are inhibited and extensors are excited. This is called crossed extensor reflex. It is due to reciprocal innervation.
Q.100 What is Babinski’s sign? When does it occur?
Babinski’s sign is the abnormal plantar reflex. In normal plantar reflex, a gentle scratch over the outer edge of the sole of the foot causes plantar flexion and adduction of all toes and dorsiflexion and inversion of the foot. But in Babinski’s sign, there is dorsiflexion of the big toe and fanning of other toes. It is common in infants due to the non-myelination of pyramidal tracts. In normal persons, it can be elicited during deep sleep. The pathological condition when it appears is upper motor lesion.
Q.101 What is clonus?
Clonus is a series of rapid and repeated jerky movements, which occur while eliciting a deep reflex. In a normal deep reflex, the contractions of a muscle or group of muscles are smooth and continuous. Clonus occurs when deep reflexes are exaggerated due to the hypertonicity of muscles in pyramidal tract lesions. Clonus is well seen in calf muscles producing ankle clonus and quadriceps producing patella clonus.
Q.102 What are pendular movements?
While eliciting a tendon jerk, some slow oscillatory movements are developed instead of brisk movements. These movements are called pendular movements and are common in the cerebellar lesion.
Q.103 What are the effects of upper and lower motor neuron lesions on reflexes?
During the upper motor neuron lesion, all the superficial reflexes are lost. The deep reflexes are exaggerated and the Babinski’s sign is positive. During lower motor neuron lesion, all the superficial and deep reflexes are lost.
Q.104 What are the segments of the spinal cord?
The spinal cord is made up of 31 segments viz.
Cervical segments = 8
Thoracic segments = 12
Lumbar segments = 5
Sacral segments = 5
Coccygeal segment = 1
Q.105 What are the neurons present in the gray horn of the spinal cord?
Anterior gray horn consists of motor neurons. The posterior gray horn consists of sensory neurons. The lateral gray horn contains intermediolateral horn cells, which give rise to sympathetic preganglionic fibers.
Q.106 Name the types of neurons present in the anterior gray horn.
Q.107 Name the types of neurons present in the posterior gray horn.
Q.108 What are the white columns of the spinal cord?
Anterior white column – between the anterior median fissure on one side and anterior nerve root and anterior gray horn on the other side
Lateral white column – between the anterior nerve root and anterior gray horn on one side and posterior nerve root and posterior gray horn on the other side
Posterior gray column – in between the posterior nerve root and posterior gray horn on one side and posterior median septum on the other side.
Q.109 Briefly classify tracts of the spinal cord.
Short tracts – connecting different parts of the spinal cord itself:
– Association or intrinsic tracts which connect the adjacent segments of the spinal cord on the same side
– Commissural tracts, which connect the opposite halves in the same segment of the spinal cord.
Long tracts or projection tracts connecting the spinal cord with other parts of the central nervous system:
– Ascending tracts which carry sensory impulses from the spinal cord to the brain
– Descending tracts, which carry motor impulses from the brain to the spinal cord.
Q.110 Enumerate the ascending tracts in the spinal cord.
Q.111 Name the type of fibers forming ascending tracts of the spinal cord.
All ascending tracts of the spinal cord are formed by the fibers of second-order neurons (crossed fibers) except posterior column tracts. The posterior column tracts are formed by the fibers of first-order neurons (uncrossed fibers)
Q.112 Which sensations are carried by these nerves?
| Fasciculus gracilis and Fasciculus cuneatus | Fine touch, tactile localization, kinesthetic movements, vibration, deep pressure. |
| Lateral spinothalamic | Pain and temperature. |
| Ventral spinothalamic | Crude touch. |
Q.113 What are the functions of spinothalamic tracts?
Anterior spinothalamic tract carries crude touch (protopathic) sensation and the lateral spinothalamic tract carries pain and temperature sensations.
Q.114 What are the functions of spinocerebellar tracts?
Ventral and dorsal spinocerebellar tracts carry subconscious kinesthetic sensation to the cerebellum.
Q.115 What are nonsensory impulses?
The impulses of subconscious kinesthetic sensation are called nonsensory impulses.
Q.116 What are the functions of posterior column tracts?
Posterior column tracts carry the impulses of:
Q.117 Classify the descending tracts of the spinal cord.
Q.118 Name the pyramidal tracts.
Q.119 Mention the origin of fibers of pyramidal tracts.
Q.120 Briefly describe the course of pyramidal tracts.
After taking origin from the cerebral cortex, the fibers of pyramidal tracts descend down through corona radiata, internal capsule, midbrain, and pons and enter the medulla. While running down through the upper part of the anterior surface of the medulla, these fibers give the appearance of a pyramid.
At the lower border of the medulla, 80% of fibers from each side cross to the opposite side forming pyramidal decussation or motor decussation. After crossing, these fibers descend through the lateral white column of the spinal cord as the lateral corticospinal tract. The remaining 20% of the fibers descend down on the same side through the anterior white column as the anterior corticospinal tract.
Q.121 What are the functions of pyramidal tracts?
Pyramidal tracts are concerned with voluntary movements of the body and are responsible for fine and skilled movements.
Q.122 What are the effects of lesion of pyramidal tracts?
Lesion in pyramidal tracts is called upper motor neuron lesion.
It causes:
Q.123 Name the extrapyramidal tracts.
Q.124 What are the functions of medial longitudinal fasciculus?
Medial longitudinal fasciculus helps in the coordination of reflex ocular movements and the integration of ocular and neck movements.
Q.125 What is the function of vestibulospinal tracts?
Vestibulospinal tracts are concerned with the adjustment of the position of head and body during angular and linear acceleration.
Q.126 What are the functions of the reticulospinal tract?
The reticulospinal tract is concerned with the control of movements, maintenance of muscle tone, respiration, and control of the diameter of blood vessels.
Q.127 What are the effects of the complete transection of the spinal cord?
Complete transection of the spinal cord causes immediate loss of sensation and voluntary movements below the level of lesion.
The effects occur in three stages:
Q.128 What is paraplegia in flexion?
During the stage of reflex activity after complete transection of the spinal cord, the tone returns to flexor muscles first. And the limbs in this condition tend to adopt a position of
slight flexion. This type of paralysis is known as paraplegia in flexion.
Q.129 What are the effects of incomplete transection of the spinal cord?
The effects of incomplete transection of the spinal cord are similar to the effects of complete transection except that, during the stage of reflex activity, the tone returns to extensor muscles first.
Q.130 What is paraplegia in extension?
During the stage of reflex activity after incomplete transection of the spinal cord, the tone returns to extensor muscles first. The limbs in this condition tend to adopt a position of slight extension. This is called paraplegia in extension.
Q.131 What is the hemisection of the spinal cord?
Injury to one lateral half of the spinal cord is called hemisection.
Q.132 What is Brown-Séquard syndrome?
The sensations carried by crossed spinothalamic tracts such as crude touch, pain, and temperature sensations are not affected. The motor changes resemble the effects of upper motor lesions.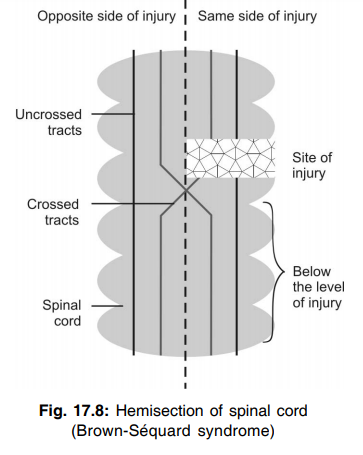
Q.134 What are the effects of hemisection of the spinal cord on the opposite side of the body below the lesion?
The sensations carried by crossed spinothalamic tracts such as crude touch, pain, and temperature sensations are lost. The sensations carried by uncrossed fibers of posterior column tracts namely, fine touch sensation, tactile localization, tactile discrimination, sensation of vibration, conscious kinesthetic sensation, and stereognosis are not affected. The motor functions are not affected. If affected, it would be mild and the effects resemble the effects of upper motor lesion.
Q.135 What are the effects of hemisection of the spinal cord on the same side of the body at the level of the lesion?
There is complete anesthesia, i.e. all the sensations are lost. The motor changes resemble the effects of lower motor lesions.
Q.136 What are the effects of hemisection of the spinal cord on the opposite side of the body at the level of the lesion?
The sensations carried by crossed spinothalamic tracts such as crude touch, pain, and temperature sensations are lost. The sensations carried by uncrossed fibers of posterior column tracts namely, fine touch sensation, tactile localization, tactile discrimination, sensation of vibration, conscious kinesthetic sensation, and stereognosis are not affected. The motor functions are not affected. If affected, it would be mild and the effects resemble the effects of lower motor lesion.
Q.137 What is syringomyelia? What is its cause?
Syringomyelia is a disease of the spinal cord characterized by the presence of fluid-filled cavities in the spinal cord. It occurs due to the overgrowth of neuroglial cells in the spinal cord accompanied by cavity formation and accumulation of fluid.
Q.138 What is dissociated anesthesia?
In the case of syringomyelia, there is loss of pain and temperature sensation whereas the sense of touch is unaffected. This condition is known as dissociated anesthesia.
Q.139 What is tabes dorsalis? What is its cause?
Tabes dorsalis is a disease of the spinal cord. It occurs due to the degeneration of dorsal nerve roots. Degeneration of dorsal nerve roots is common in syphilis.
Q.140 What is the feature of tabes dorsalis?
The characteristic feature of tabes dorsalis is the slow progressive nervous disorder affecting the motor and sensory functions of the spinal cord.
Q.141 Classify sensations.
• Somatic sensations:
– Epicritic or light sensations
– Protopathic or crude sensations
– Deep sensations.
• Special sensations:
– Visual sensation
– Auditory sensation
– Gustatory or taste sensation
– Olfactory sensation or sensation of smell.
Q.142 Name the epicritic sensations.
Q.143 Name the protopathic sensations.
Q.144 Name the deep sensations.
Q.145 How are the sensations from the face transmitted to the brain?
Through the ophthalmic, maxillary, and mandibular divisions of the trigeminal nerve.
Q.146 What is the somatosensory system?
The somatosensory system is the sensory system involving the pathways, which convey the information from the sensory receptors present in the skin, skeletal muscles, and joints.
Q.147 Name the components of somatosensory pathways.
Q.148 Define the following.
Anesthesia: Loss of all sensations
Hyperesthesia: Increased sensitivity to sensory stimuli
Hypesthesia: Reduction in the sensitivity to sensory stimuli
General anesthesia: Loss of all sensations with loss of consciousness produced by anesthetic agents.
Analgesia: Loss of pain sensation
Hyperalgesia: Increased sensitivity to pain stimulus
Illusion: Mental depression due to misinterpretation of a sensory stimulus
Hallucination: Feeling of a sensation without any stimulus.
Q.149 What are lemnisci? Name the different lemnisci.
The prominent bundles of sensory nerve fibers in the brain are called lemnisci.
Different lemnisci:
| Spinal lemniscus formed by spinothalamic tracts |
| Lateral lemniscus formed by fibers carrying the sensation of hearing from cochlear nuclei to the inferior colliculus and medial geniculate body |
| Medial lemniscus formed by posterior column tracts |
| Trigeminal lemniscus formed by fibers of sensory nuclei of the trigeminal nerve. |
Q.150What is the lateral motor system? Name its components.
The lateral motor system is the part of the motor system formed by the motor nerve fibers, which terminate on motor neurons situated in the lateral part of the ventral gray horn in the spinal cord and also on the corresponding motor neurons of cranial nerve nuclei in the brainstem.
It includes:
Q.151 What are the functions of the lateral motor system?
Q.152 What is the medial motor system? Name its components.
The medial motor system is the part of the motor system formed by the motor nerve fibers which terminate on the motor neurons situated in the medial part of the ventral gray horn of the spinal cord and on the corresponding motor neurons of cranial nerve nuclei in the brainstem.
It includes:
Q.153 What are the functions of the medial motor system?
Q.154 What are upper motor neurons? Name them.
The neurons in the higher center of the brain, which control the lower motor neurons are called upper motor neurons.
Upper motor neurons are:
Q.155 What are the lower motor neurons? Name them.
Lower neurons are the anterior horns cells in the spinal cord and motor neurons of the cranial nerve nuclei situated in the brainstem, which innervate the skeletal muscles directly. These neurons constitute the ‘Final common pathway” of the motor system. The lower motor neurons are the alpha motor neurons in the anterior horns of the spinal cord and the cells of nuclei of III, IV, V, VI, VII, IX, X, XI, and XII cranial nerve.
Q.156 What are the effects of upper motor neuron lesions?
Q.157 What are the effects of lower motor neuron lesion?
Q.158 What are the main differences between upper and lower motor neuron lesions?
| LMNL | UMNL |
| Single individual muscle is affected | Group of muscles are affected. |
| Flaccid type of muscle paralysis due to hypotonia | Spastic type of muscle paralysis due to hypertonia |
| Disuse atrophy of muscle takes place | Not severe |
| All reflexes are absent as the motor pathway is damaged | Deep reflexes are hyperactive due increased g motor activity and some superficial reflexes like abdominal, cremasteric reflexes are lost. |
| Babinski’s sign is Negative | It is positive. |
Q.159 What are the components of pain sensation?
Q.160 Name the nerve fibers transmitting pain sensation.
Fast pain is transmitted by type A delta afferent fibers and slow pain is transmitted by type C fibers.
Q.161 What are the causes of visceral pain?
Q.162 What is referred pain?
The pain sensation, produced in some parts of the body is felt in other structures away from the place of development. This is called referred pain.
Q.163 Give some examples of referred pain.
Q.164 Name the neurotransmitter involved in pain sensation.
Substance P
Q.165 What is analgesia system?
The pain control system of the central nervous system is called the analgesia system. It inhibits the impulses of pain sensation.
Q.166 What are the pain control systems in the brain and spinal cord?
The pain control system in the brain is present in gray matter surrounding the aqueduct of Sylvius and raphe Magnus nuclei in the pons. In the spinal cord, the pain control system is in the posterior gray horn which is considered as a gateway for pain impulses.
Q.167 What is the gate theory of pain?
When pain sensation is produced in any part of the body, along with pain fibers, some of the other afferent fibers particularly the touch fibers reaching the posterior column of the spinal cord are also activated. The posterior column of the spinal cord sends collaterals to cells of substantia gelatinosa in the posterior gray horn. Thus, some of the impulses ascending via posterior column fibers pass through the collaterals and reach substantia gelatinosa. Here, the impulses inhibit the release of substance P by pain fibers, and pain sensation is suppressed. Thus, there is a gating of pain in the posterior gray horn level.
Q.168 Name important centers or nuclei present in medulla oblongata.
Q.169 What are the important structures present in pons?
Q.170 What are the important structures present in the midbrain?
Q.171 What is the red nucleus? What is its function?
The red nucleus is a large oval or round mass of gray matter between the superior colliculus and the hypothalamus.
It controls:
Q.172 Name the different groups of thalamic nuclei.
Q.173 What are the functions of the thalamus?
Thalamus form:
Q.174 What is thalamic syndrome? What are its features?
The signs and symptoms that occur during thalamic lesion are together called thalamic syndrome. The features are:
Q.175 What is the cause of thalamic lesions?
Thalamic lesion occurs mostly because of the blockage of thalamogeniculate branch of the posterior cerebral artery by thrombosis.
Q.176 What is tremor? Which type of tremor occurs in thalamic syndrome?
Rapid alternate rhythmic and involuntary movement of flexion and extension in the joints of fingers and wrist or elbow is called tremor. In thalamic syndrome, intension tremor (tremor while attempting to do any voluntary act) occurs.
Q.177 What is the internal capsule? Where is it situated?
The internal capsule is the compact band of afferent and efferent fibers connecting the cerebral cortex with the brainstem and spinal cord. It is situated in between the thalamus and caudate nucleus on the medial side and lenticular nucleus on the lateral side.
Q.178 What are the nuclei of the hypothalamus?
| Anterior or preoptic group – preoptic nucleus, paraventral nucleus, anterior nucleus and supraoptic nucleus |
| Middle or tuberal group – dorsomedial nucleus, ventromedial nucleus, lateral nucleus and arcuate (tuberal) nucleus |
| Posterior or mammillary group – posterior nucleus and mammillary body. |
Q.179 Enumerate the functions of the hypothalamus.
Q.180 What is the role of hypothalamic centers for regulation of body temperature?
Q.181 What is the role of the hypothalamus in the regulation of food intake?
Hypothalamus has two centers to regulate the food intake, the feeding center, and satiety center. Normally, the feeding center is active and it is controlled by the satiety center.
Q.182 Name the mechanisms involved in the regulation of appetite and food intake.
Q.183 What is the role of the hypothalamus in the regulation of water balance?
Hypothalamus regulates water balance by two mechanisms:
Q.184 Name the hypothalamic centers concerned with behavior and emotional changes.
Q.185 What is rage? What is sham rage?
When punishment center is stimulated in animals, a violent aggressive emotional state is exhibited. This is called rage. It includes the reactions like development of defense posture, extension of limbs, lifting of tail, hissing, spitting, and severe savage attack even by mild provocation. Normally the punishment center in hypothalamus is kept inhibited by cortical centers. So mild irritations are overcome or ignored. However, in animals or human beings with brain lesions, even a very mild stimulus can evoke violent and angry reactions of rage. This type of rage is called sham rage. It is due to release of hypothalamus from cortical control.
Q.186 Name the disorders caused by hypothalamic lesions.
Q.187 What is diabetes insipidus? What is its cause?
Diabetes insipidus is the disease characterized by excretion of large quantity of dilute urine. It is due to the failure of water reabsorption from renal tubules. It occurs due to deficiency or absence of ADH because of tumor of the hypothalamus.
Also read: Nervous System Part 2 (Viva)
Comments (0)