Hard and Soft Palate
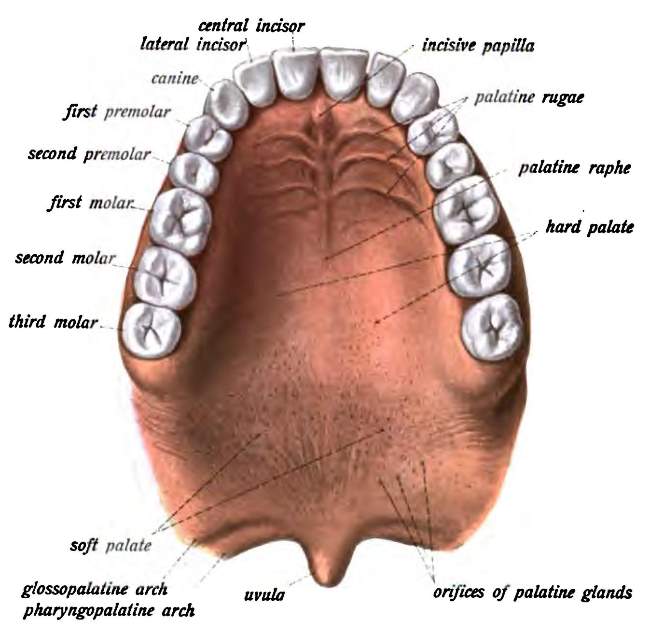
Hard palate
It forms the partition between the nasal & oral cavities.
Formation of Hard Palate
Anterior 2/3rd - formed by the palatine process of the maxilla
Posterior 1/3rd - formed by horizontal plates of palatine bone
Lining epithelium above the Hard palate
Pseudostratified ciliated columnar epithelium (respiratory epithelium)
Lining epithelium below the hard palate
Non-keratinized stratified squamous epithelium
Soft palate
It is the muscular fold suspended from the posterior border of the hard palate
It separates the nasopharynx from oropharynx
Muscles of the soft palate
- Tensor veli palatini
- Levator veli palatini
- Musculus uvulae (Muscle of uvula)
- Palatoglossus
- Palatopharyngeus
Notes: Tonsillar fossa is bounded anteriorly by palatoglossus & posteriorly by palatopharyngeus.
Palatoglossus is also regarded as the muscle of tongue
Palatopharyngeus is also regarded as a longitudinal muscle of the pharynx.
Artery supply of soft palate:
- Greater palatine branch of the maxillary artery
- Ascending palatine branch of the facial artery
- Palatine branch of ascending pharyngeal artery
Note: Maxillary, facial, and ascending pharyngeal arteries are branches of the external carotid artery.
The blood supply of the palatine tonsil, soft palate, and pharynx is quite similar.
Nerve supply of soft palate:
Motor Supply-
All the muscles of the soft palate are supplied by the cranial root of the accessory nerve through the vagus nerve except tensor veli palatini which is supplied by the mandibular nerve (nerve of 1st pharyngeal arch)
Secretomotor supply by branches from the pterygopalatine ganglion
Sensory supply-
Maxillary nerve and glossopharyngeal nerve
Function of the soft palate
- It closes the mouth from the oropharynx during chewing, so that breathing is unaffected.
- It separates the oropharynx from the nasopharynx during swallowing so that food doesn’t enter the nose.
Development of Palate
- Premaxilla/ Primitive palate carrying upper four incisor teeth is formed by the fusion of right and left medial nasal folds, which are derived from frontonasal prominence
- Rest of the palate (secondary palate) is formed by the palatine process of the maxilla & horizontal plates of palatine bones, which are derived from maxillary prominence
Most of the palate gets ossified to form the hard palate.
However the unossified part of the fused palatal process forms the soft palate.
Notes:
The soft palate comprises epithelium, connective tissue & muscles.
- The epithelium is from the ectoderm of the maxillary process.
- The muscles are derived from 1st (tensor veli palatini), 4th & 6th bronchial arch and accordingly are innervated by the mandibular nerve and cranial root of the accessory nerve through the vagus
Vagus nerve contains fibers from the cranial root of the accessory nerve.
Maxilla (upper jaw) is developed from maxillary prominence
Intermaxillary segment:
The structure formed by the fusion of right and left medial nasal prominence, which has been derived from frontonasal prominence is called the intermaxillary segment
Clinical Anatomy:
|
1) Cleft lip:
It is due to the failure of the union of the medial nasal prominence with the maxillary processes
|
2) Cleft Palate
It is a congenital defect caused by non-fusion of right & left palatal processes. |
|
3) Soft palate is elevated during swallowing to shut off the nose & thus it prevents the food from entering the nose.
But in the case of soft palate paralysis, this function is impaired & nasal regurgitation of foods occurs during swallowing.
|
|
4) The soft palate is innervated by the vagus nerve.
The contraction of the levator veli palatini raises the soft palate.
When the vagus nerve is injured, the soft palate becomes paralyzed & nasal regurgitation of food occurs through the nose.
|
Comments (0)