ICD 10 code for Pleural Effusion
3 years ago 5041
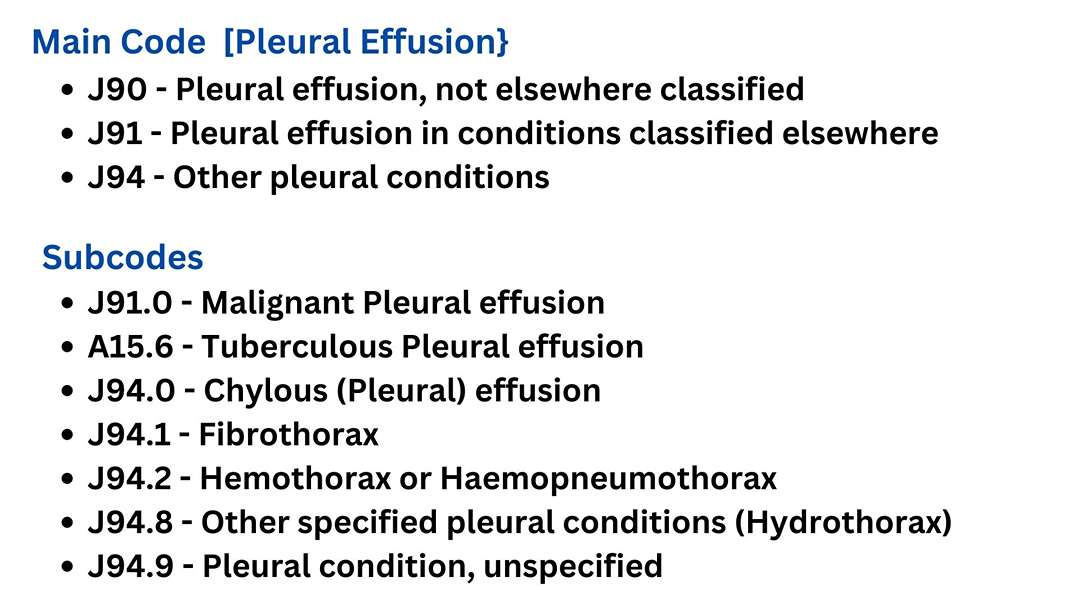
J90 is the primary ICD-10 code for pleural effusion. It is used to indicate the presence of pleural effusion, which is the accumulation of excess fluid in the pleural cavity surrounding the lungs.
From J90 to J94 ICD 10 code is related to pleura diseases. These include:
J90 is the ICD 10 code for Pleural effusion, not elsewhere classified. This is also applicable to Pleurisy with effusion. Parapneumonic pleural effusion also comes under the J90 ICD 10 code. J90 ICD code is not applicable to:
Under the J91 ICD 10 code, the subcode J91.0 is the ICD 10 code for Malignant Pleural effusion.
ICD-10 provides additional subcodes under J94 to specify different types, causes, and characteristics of pleural effusion. Some of these subcodes include:
J94.8 is the ICD 10 code for Hydrothorax or hydropneumothorax. Hydropneumothorax means collection of both air and blood within the pleural cavity. Fibrothorax means fibrosis of the pleura. The ICD 10 code for fibrothorax is J94.1. Chylous effusion means accumulation of milky white chyle due to obstruction/disruption of the thoracic duct in the pleural cavity.
Traumatic haemopneumothorax & traumatic haemothorax are not included in the J94 ICD 10 code. S27.2 is the ICD 10 code for Traumatic haemopneumothorax and S27.1 is the ICD 10 code for traumatic haemothorax.
Use of Subcodes:
The subcodes help provide more specific information about the nature and cause of the pleural effusion. For example, J91.0 is used when the pleural effusion is due to malignancy, while J90 is a more general code for pleural effusion not elsewhere classified.
When coding for pleural effusion, it's essential to use the most accurate and specific code based on the patient's diagnosis and medical documentation. Proper coding is crucial for billing, research, and healthcare planning. Always refer to the most current version of the ICD-10 for accurate coding.
In summary, J90 is the commonly used ICD 10 code for pleural effusion, not elsewhere classified. J90 is also the ICD 10 code for Parapneumonic pleural effusion. J91.0 is the ICD 10 code for Malignant Pleural effusion. A15.6 is the ICD 10 code for Tuberculous Pleural effusion. Pneumonia, Malignancy & tuberculosis are the main causes of pleural effusion. So the ICD 10 code of pleural effusion under those heading are more important.
|
Pleural Effusion is an abnormal accumulation of excessive fluid in the pleural cavity. Normally, the pleural cavity contains about 5 - 15 ml of pleural fluid. At least 500 ml of pleural fluid should be accumulated to be clinically detected. And at least 200 ml of pleural fluid should be present to be detectable by X-ray.
The most common causes of unilateral pleural effusion are
Other causes of pleural effusion are
Examination of the respiratory system reveals the following findings.
The pleural effusion and pneumothorax can be clinically differentiated by percussion. Percussion note is stony dull in pleural effusion and hyper resonance in case of pneumothorax.
Following are the radiological chest x-ray findings of pleural effusion.
Investigation done in pleural effusion are:
In pleural fluid study, physical, cytological, biochemical, and microbiological examinations are done.
On physical examination of pleural fluid, a cloudy appearance of pleural fluid is seen in para pneumonia effusion. The straw color of pleural fluid in TB and the hemorrhagic appearance of pleural fluid in malignancy can be found.
On cytological examination, there will be increased WBC with predominant neutrophil in parapneumonic effusion. In TB and malignancy, there will be increased WBC with predominant lymphocytes.
On biochemical examination, there is increased protein in exudative effusion and decreased glucose in para-pneumonic and tubercular effusion. Additionally, there may be increased ADA in Tubercular effusion.
On microbiological examination, pyogenic organisms can be found in para-pneumonic effusion and acid-fast bacilli in Tubercular effusion.
Therapeutic aspiration of the pleural fluid can be done to reduce breathlessness and other complications. However not more than 1.5 liters of pleural fluid is aspirated at a time. If a large amount of fluid is aspirated at a time there may be re-expansion pulmonary edema and sudden mediastinum shifting that can cause severe pain and shock.
The mainstay of management of pleural effusion is the treatment of underlying causes i.e. pneumonia, TB, and malignancy.
The treatment of Tubercular Pleural Effusion includes
Comments (0)