Multiple Myeloma
4 years ago 1974
Multiple myeloma is a malignant proliferation of plasma cells. Multiple myeloma is a chronic, progressive and fatal malignant condition in which the fundamental abnormality is a neoplastic proliferation of plasma cells that infiltrate the bone marrow and often other body tissues.
It comes under immunoproliferative disorder.
There are 3 major types of Proliferative disorders.
IMMUNOPROLIFERATIVE DISORDER:
Disorders characterized by abnormal proliferation of immunoglobulin-producing cells and abnormal proliferation of immunoglobulin monoclonal (M protein)represent part of the spectrum of disease due to the neoplastic behavior of the B lymphocyte series.
It is defined as a group of disorders arising from the abnormal proliferation of a single clone of immunoglobulin-secreting cells giving rise to paraproteinaemia.
Classification of Immunoproliferative Disorder:
A. Plasmacytic:
| Benign: Benign monoclonal gammopathy Essential cryoglobulinemia |
| Malignant: Multiple myeloma Solitary plasmacytoma Plasma cell leukemia |
| Nature unknown: Heavy chain disease Light chain disease |
B. Lymphocytic:
Benign:
Malignant:
C. Others:
Paraproteinaemia is a disorder characterized by abnormal proliferation of immunoglobulin-producing cells due to the neoplastic behavior of B-Lymphocytic series with an increase in serum level of homogenous immunoglobulin (monoclonal IG) or its fragments.
Paraprotein is the presence of a monoclonal immunoglobulin band (M-band) in the serum. It reflects the synthesis of immunoglobulin from a single clone of plasma cells.
Causes of paraproteinemia:
Multiple myeloma is a chronic, progressive and fatal malignant condition in which the fundamental abnormality is a neoplastic proliferation of plasma cells that infiltrate the bone marrow and often other body tissues.
It is a malignant proliferation of plasma cells.
|
Plasma cells are derived from B lymphocytes and produce immunoglobulin (Ig) which contains heavy and light chains. Normally Ig molecule consists of 4 polypeptide chains 2 heavy chains and 2 light chains.
Each Ig molecules have either 2 kappa or 2 lambda light chains. In myeloma, plasma cells produce monoclonal (M) Ig of a single heavy and light chain commonly referred to as a paraprotein. The most common abnormality is the production of excess of light chains over heavy chains. The excess light chains are secreted into the extracellular fluid and readily pass through the glomerulus. Light chains are catabolized by renal tubular cells but when present in excess pass into the urine as Bence Jones Protein. The most common monoclonal Ig (M protein) is:
|
Clinical features of Multiple Myeloma developed due to tissue infiltration, production of a large number of paraprotein, and impairment of immunity.
Myeloma is a disease of middle and old age (50-70 years), male predominance.
1. Bone:
(Bone becomes soft due to infiltration and proliferation of myeloma cells causing destruction of medullary and cortical bone and causing osteolysis due to increased osteoclastic activity by a factor released by myeloma cells).
2. Anemia: Due to the dilutional effect of a large amount of paraprotein in circulation, depression of erythropoiesis by infiltration of myeloma cells in the bone marrow, and the effects of cytotoxic drugs.
3. Infection: Due to subnormal levels of normal Ig and suppression of the normal antibody
4. Bleeding manifestation: Due to platelets suppression and paraprotein causes abnormal platelets function
5. Renal insufficiency: Due to the deposition of antibody-derived materials in the kidney
6. Nervous system manifestations like quadriplegia, and paraplegia due to compression by collapsed vertebrae or myeloma tissue.
1. Routine blood examination:
2. Peripheral blood film: (Shows leucoerythroblastic blood picture with an abnormally blue-stained background in the blood film).
3. Bone marrow examination:
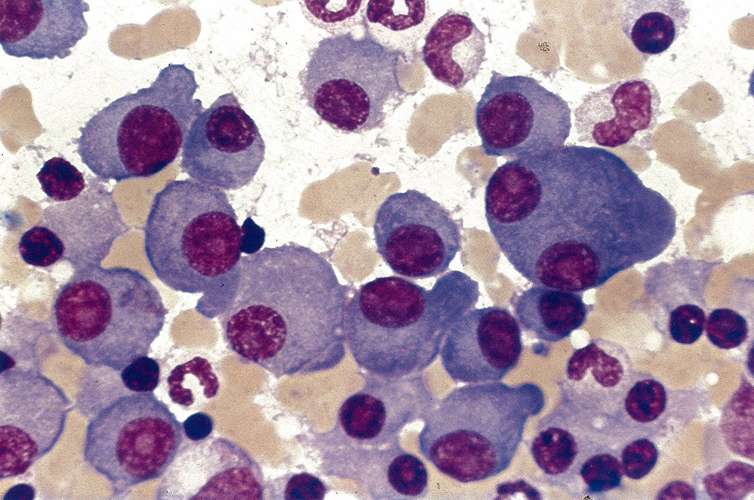
Fig: Clusters of plasma cells in multiple myeloma in bone marrow smear
4. Biochemical findings:
5. Electrophoresis:
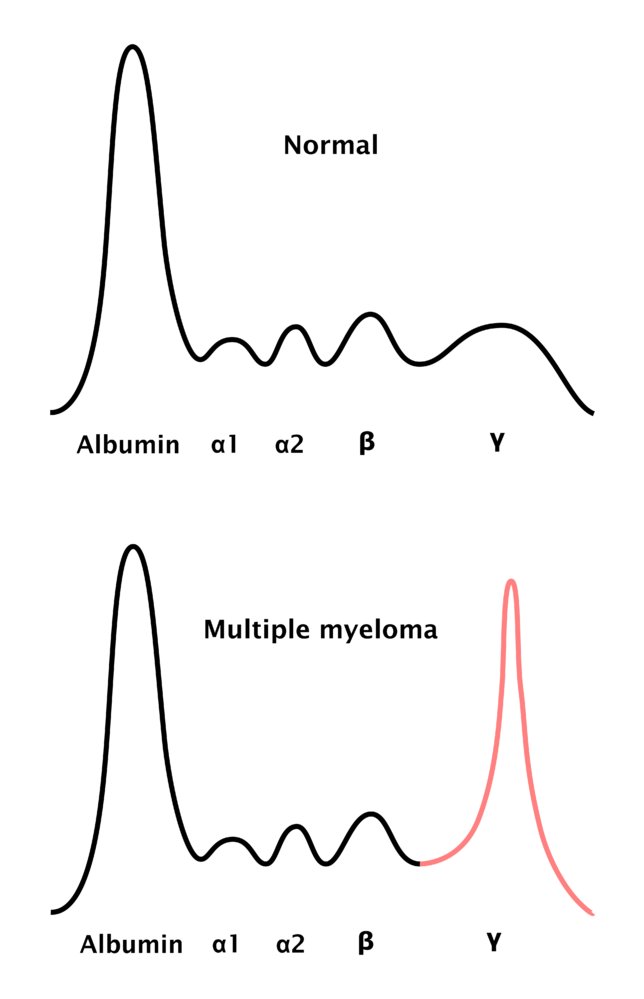
Fig: Electrophoresis in multiple myeloma - the monoclonal antibodies cause a peak in the gamma-globulin zone of the electrophoresis, which is termed M protein (also M component, myeloma protein, spike protein, and paraprotein).
6. Urine examination:
Detection of Bence Jones Protein in urine.
7. Radiological findings:
Osteolytic lesions appear as multiple rounded discrete punched-out areas with no sclerosis at the margin. They occur most frequently in bones normally containing red marrow, particularly in the skull and pelvic bones.

Fig: Multiple punched-out lytic lesions in X-ray skull of a patient with a history of multiple myeloma
1. Osteolytic lesion in bone (Seen on X-ray)
2. Detection of monoclonal protein (M protein or paraprotein in serum or urine).
3. Increased proliferation of plasma cells with immature form in bone marrow
Causes of increased plasma cells in bone marrow:
It is an immunoglobulin light chain either kappa or lambda, excreted in urine and found in various pathological conditions.
Free monoclonal kappa or lambda light chain of immunoglobulin appears in the urine as Bence Jones Protein.
Properties of Bence Jones Protein:
Detection of Bence Jones Protein:
Bence Jones Protein Found in:
|
Heat precipitation test/ Fluctuation test:
Read also
A vape clutch is a type of vape mod that is designed to be sleek and compact, making it easy to carry around in a pocket or purse. It typically features a single battery and a simple button mechanism to activate the device. The small size of a vape clutch makes it an ideal choice for vapers who are always on the go and need a device that is easy to transport. However, the compact size of a vape clutch can also limit the battery life and overall power of the device compared to larger mods. Vape clutches come in a variety of designs and colors, making it easy for vapers to find one that suits their personal style
Comments (0)