Would healing
3 years ago 1141
Wound healing, also called Tissue Repair, refers to the restoration of tissue architecture and function after an injury.
Wound healing occurs in two ways:
Definition of Regeneration: Regeneration is the Process of replacement of the damaged components by (proliferation of residual cells and maturation of tissue stem cells) similar tissue and essentially return to a normal state.
Type of cells that undergo regeneration:
Scar formation:
Definition of scar formation: Repair occurs by the laying down of connective (fibrous) tissue, is called scar formation.
If the injured tissues are incapable of regeneration, or if the supporting structures of the tissue are too severely damaged to support the regeneration of the tissue cells, repair occurs by the laying down of connective (fibrous) tissue, a process that may result in scar formation.
Both regeneration and scar formation processes involve
Types of cells involved in wound healing
Lots of cells proliferate during wound healing
Stem cells
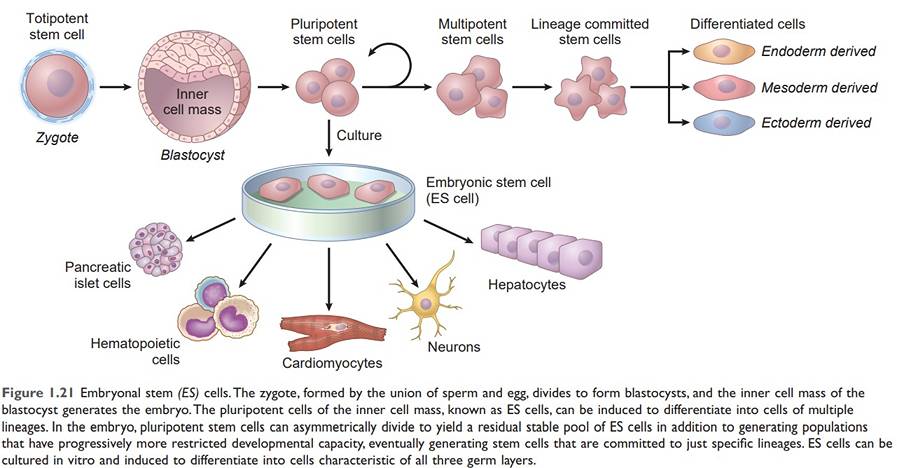
Stem cells are specialized, undifferentiated, or partially differentiated cells that can differentiate into various types of cells and proliferate indefinitely to produce more of the same stem cell.
Steam cell category
During development, totipotent stem cells can give rise to the full range of differentiated tissues;
In the mature organism, adult stem cells only have the capacity to replace damaged cells and maintain cell populations within the tissues where they reside.
Embryonic stem cell
ESCs derived from the inner mass of the blastocyst prior to implantation lasting for 4th to 7th day and disappear after the 7th day. Embryonic stem (ES) cells are the most undifferentiated. They are present in the inner cell mass of the blastocyst, have virtually limitless cell renewal capacity, and can give rise to every cell in the body; they are thus said to be totipotent.
Adult stem cells (Tissue stem cells)
Stem cells are present inside different types of tissue:
Growth factors:
Growth factors are polypeptides that drive the proliferation of many cell types.
The function of Growth factor:
Growth factors and receptors
Growth factors bind to specific receptors and, ultimately, influence the expression of genes that:
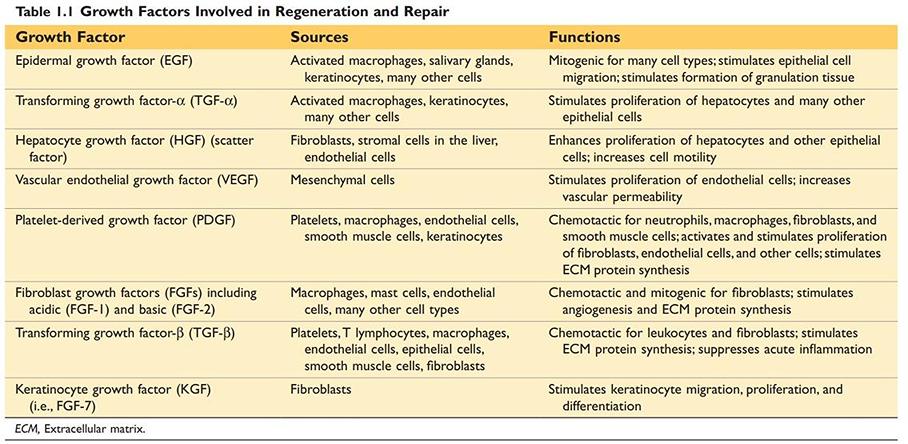
Growth Factors Involved in Regeneration and Repair
Source: Robbin’s 10th Edition (Page 20)
Extracellular Matrix:
The ECM is a protein network that constitutes a significant proportion of any tissue.
Cell interactions with the ECM are critical for the development, healing, and maintenance of normal tissue architecture.
The function of Extracellular matrix:
Extracellular matrix occurs in two basic forms:
Components of Extracellular matrix
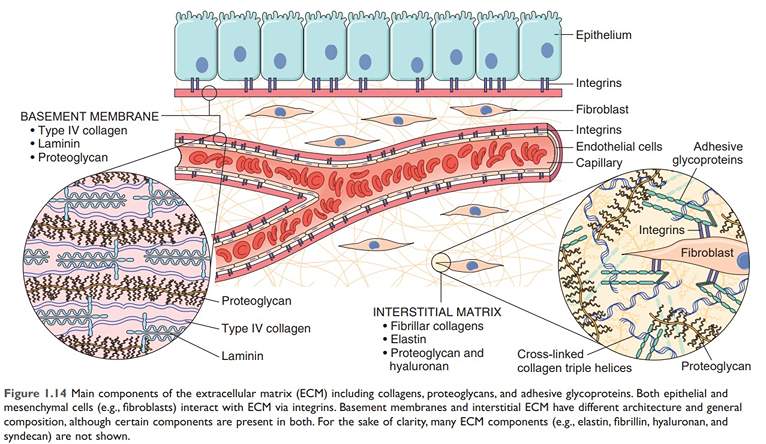
Figure: Major Components of ECM
Source: Robbin’s 10th Edition (Page 23)
The sequence of events that results in cell division is called the cell cycle.
Phases of Cell cycle:
There are 4 Phases of the cell cycle.
G0 (Gap 0): Quiescent cells that are not actively cycling are said to be in the G0 state
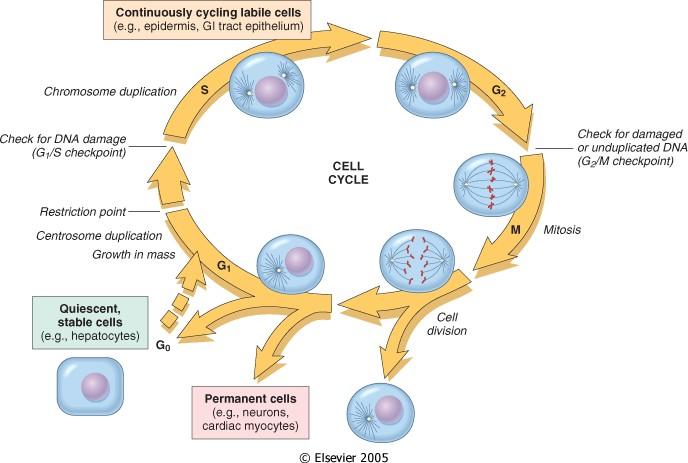
Figure: Cell cycle
Source: Robbin’s 10th Edition (Page 26)
Regulation of Cell cycle:
Progression is driven by proteins called cyclins and cyclin-associated enzymes called cyclin-dependent kinases (CDKs)
Function: enforcing the cell cycle checkpoints
Types of cell cycle checkpoints:
The function of cell cycle checkpoints:
G1/S checkpoint (restriction point):
Cell checks whether it has enough raw material to fully reduplicate its DNA. An unhealthy of malnourished cell will get stuck at this point.
G1/M checkpoint (restriction point):
Check for damaged or unduplicated DNA
When cells detect DNA irregularities, checkpoint activation delays cell cycle progression and triggers DNA repair mechanisms. If the genetic derangement is too severe to be repaired, cells either undergo apoptosis or enter a non-replicative state called senescence—primarily through p53-dependent mechanisms
Cellular proliferation
Cell proliferation is fundamental to the development, maintenance of steady-state tissue homeostasis, and replacement of dead or damaged cells.
Key elements needed for normal cellular proliferation:
On the basis of proliferative activity, tissues of the body are divided into three groups
A. Continuously dividing (labile) tissues:
Cells proliferate throughout life. They are derived from stem cells, self-renewal, and differentiation (regenerate).
Example of labile tissue or continuously dividing tissues:
B. Stable cell:
Cells of these tissues are quiescent (G0 stage) and have limited ability to replicate. Can undergo rapid division in response to stimuli.
Examples of stable cells:
C. Permanent cell:
Examples of permanent cells: Neurons, skeletal muscle, and cardiac muscle
Cells and tissue Regeneration in wound healing:
Regeneration involves:
Regeneration of the liver is a classic example of repair by regeneration.
Regeneration of the liver may occur by:
The proliferation of hepatocytes occurs after partial hepatectomy. Resection of up to 90% of the liver can be corrected by the proliferation of the residual hepatocytes. Proliferation of hepatocytes is triggered by cytokines and growth factors produced in response to the loss of liver mass and inflammation.
In the first, or priming phase, Cytokines such as IL-6 produced mainly by Kupffer cells act on hepatocytes.
In the second, or growth factor, phase, Growth factors such as hepatocyte growth factor (HGF) and TGF-α, produced by many cell types, act on primed hepatocytes to stimulate cell metabolism and entry of the cells into the cell cycle.
It takes several hours to enter the cell cycle, progress from G0 to G1, and reach the S phase of DNA replication.
In the final, termination phase: Hepatocytes return to quiescence. Anti-proliferative cytokines of the TGF-β family are likely involved.
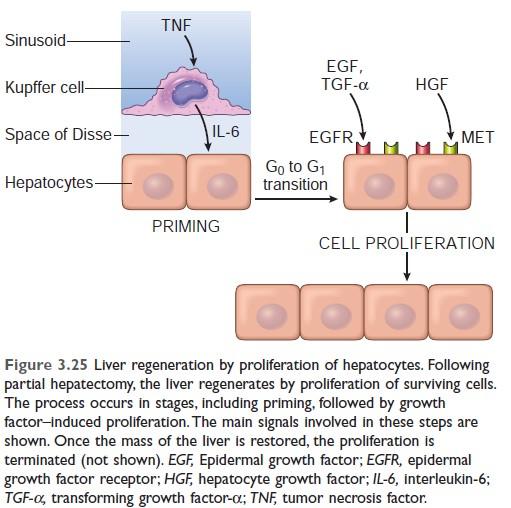
Mechanism of liver regeneration (Robbin's 10th edition)
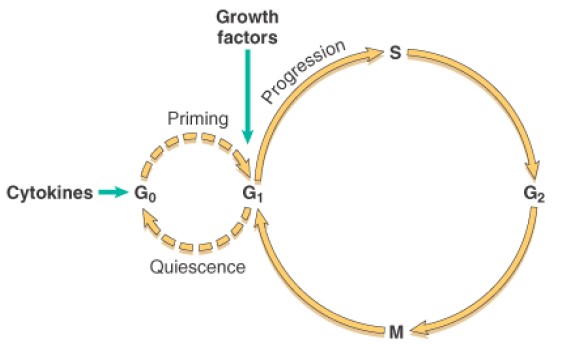
Mechanism of liver regeneration
Robbin’s 7th Edition
Angiogenesis is the process of new blood vessel development from existing vessels.
Steps of angiogenesis
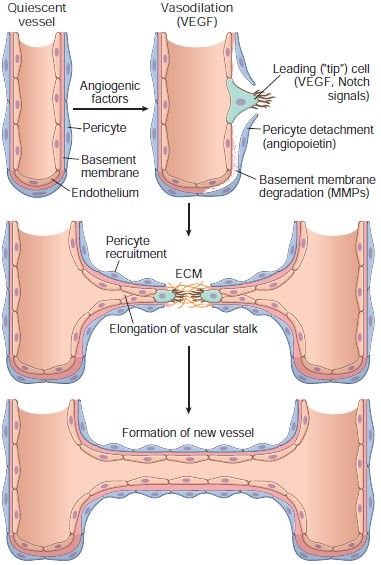
Figure: Steps of angiogenesis
The Specialized type of tissue formed by migration and proliferation of fibroblast and deposition of loose connective tissue, together with the vessels and interspersed mononuclear leukocytes is called granulation tissue. Granulation tissue is the hallmark of healing.
Characteristics of granulation tissue:
Histologic features of granulation tissue:
Granulation tissue is characterized by
Source: Robbin’s 10th Edition (Page 106)
Examples of wound healing and Fibrosis
Two clinically significant types of wound healing/repair
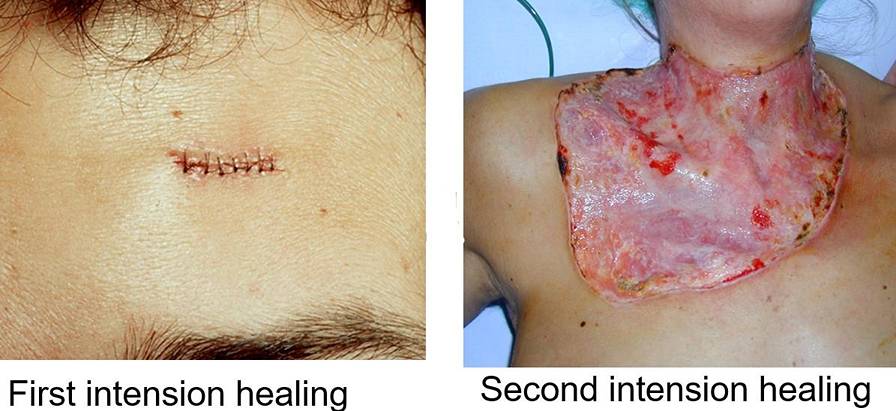
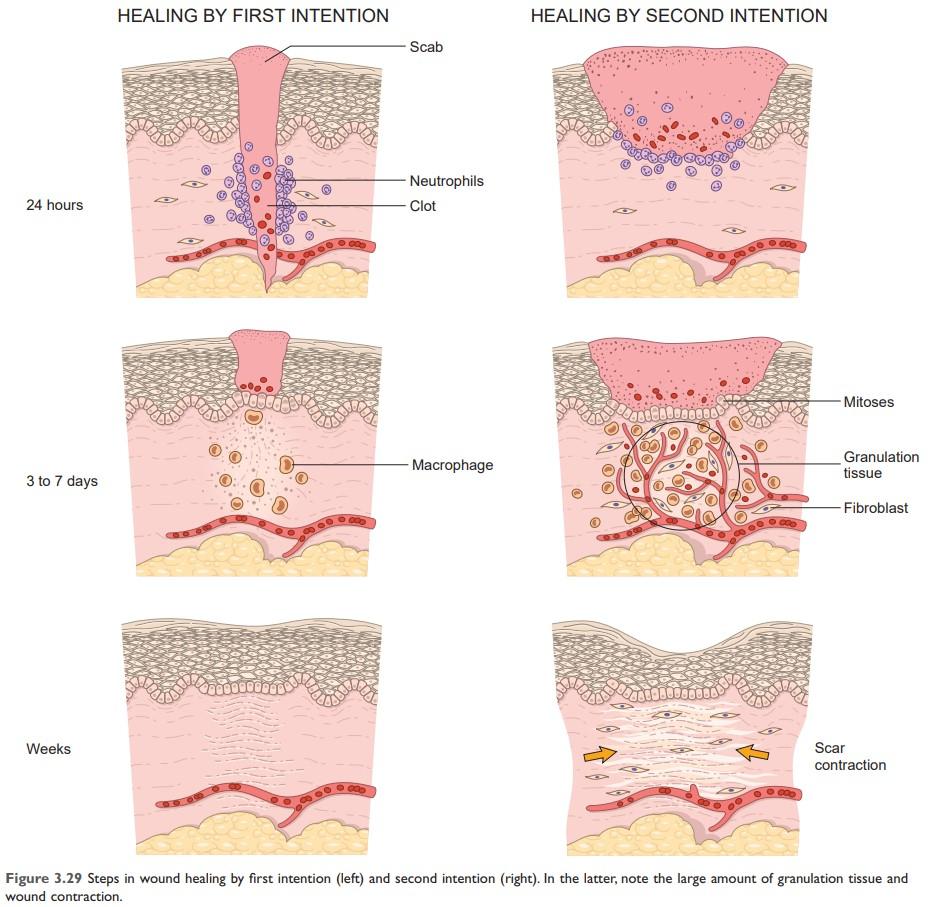
Healing of Skin Wounds
Based on the nature and size of the wound, Skin wound healing classically occur by
Criteria of Primary wound healing or First intention healing:
The repair consists of the same three connected processes that we have described previously:
Example of Primary wound healing or First intention healing:
Healing of a clean, uninfected surgical incision approximated by surgical sutures.
Secondary wound healing is also called healing by the secondary union. When cell or tissue loss is extensive, then wound healing occurs by secondary wound healing.
Secondary wound healing occurs by involving a combination of regeneration and scarring.
Example of secondary wound healing:
Large wounds, abscesses, ulceration, infarction in parenchymal organ
Primary wound healing occurs in the small cut wounds, while secondary wound healing occurs in wounds causing large tissue deficits
The fibrin clot is larger, and there is more exudate and necrotic debris in the wounded area in secondary wound healing than in primary wound healing. Inflammation is more intense in secondary wound healing. Large defects have a greater potential for secondary, inflammation-mediated injury in secondary wound healing.
Much larger amounts of granulation tissue are formed, resulting in a greater mass of scar tissue in secondary wound healing than in primary wound healing
Wound contraction occurs in secondary intention healing (as there is a large gap in the wound) by modified fibroblasts (myofibroblasts). But in primary wound healing wound contraction does not occur.
Connective tissue deposition in wound healing
Scar formation: Repair by connective tissue deposition.
Fibrosis:
The term fibrosis is often used to describe the deposition of collagen that occurs:
Organization: If fibrosis develops in a tissue space occupied by an inflammatory exudate, it is called organization (as in organizing pneumonia affecting the lung).
Wound healing by connective tissue deposition: Steps in scar formation
A. Immediately after the following injury,
The narrow incisional space fills with clotted blood containing fibrin and blood cells.
B. Within 24 hours:
C. Within 24 to 48 hours:
Epithelial cells from both edges have begun to migrate and proliferate along the dermis yielding a thin but continuous epithelial layer that closes the wound.
D. By day 3
E. By day 5
F. During the second week:
G. By the end of the first month:
| Macrophages release matrix metalloproteinases and collagenases (require zinc), which facilitate the final remodeling of type III collagen into type I collagen. Collagen becomes more organized, returning strength to the region of injury. Peak tensile strength (∼ 80% of original strength) is reached ∼ 60 days after injury. Sweat and sebaceous glands do not regenerate. |
Source: Robbin’s 10th Edition (Page 109)
Remodeling of connective tissue in wound healing
Wound contraction helps to close the wound by decreasing the gap between its dermal edges and by reducing the wound surface area.
Primary healing differs from secondary healing is the phenomenon of wound contraction. Wound contraction involves the formation of a network of myofibroblasts, which are modified fibroblasts that have contractile properties. Within 6 weeks, large skin defects may be reduced to 5% to 10% of their original size, largely by contraction.
1) Systemic Factors influencing wound healing:
A. Nutrition:
B. Metabolic status:
C. Circulatory status
D. Hormones, such as glucocorticoids,
2) Local factors influence wound healing:
A. Infection: The most important cause of delay in healing due to persistent tissue injury and inflammation.
B. Mechanical factors The early motion of wounds, can delay healing, by compressing blood vessels and separating the edges of the wound.
C. Foreign bodies such as unnecessary sutures or fragments of steel, glass, or even bone, constitute impediments to healing.
D. Size, location, and type of wound:
1) Inadequate formation of granulation tissue or deficient scar formation:
Wound dehiscence or rupture:
Most common after abdominal surgery, due to increased abdominal pressure. This mechanical stress can be generated by vomiting, coughing, or ileus
Ulceration:
2) Excessive formation of the repair components:
3) Formation of contracture
4) Cicatrization
5) Painful scar
6) Squamous cell carcinoma

Figure: Diabetic leg ulcer
Excessive Scarring:
Excessive formation of the components of the repair process can give rise to hypertrophic scars (occur within the boundary of the wound) and keloids (Beyond the wound boundary).
The accumulation of excessive amounts of collagen may give rise to a raised scar known as a hypertrophic scar. It occurs within the boundaries of the wound.

Figure: Hypertrophic scar
If the scar tissue grows beyond the boundaries of the original wound and does not regress, called a keloid. More common among African-Americans for unknown reasons. The mechanisms of keloid formation are still unknown.
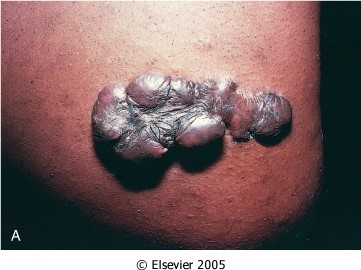
Figure: Keloid

Figure: Keloid
Proud flesh or exuberant granulation:
Formation of excessive amounts of granulation tissue, which protrudes above the level of the surrounding skin and blocks re-epithelialization known as exuberant granulation (or, with more literary fervor, proud flesh).

Figure: Exuberant granulation
Finally (fortunately rarely), incisional scars or traumatic injuries may be followed by exuberant proliferation of fibroblasts and other connective tissue elements that may recur after excision. called desmoids, or aggressive fibromatoses.
Formation of contracture:
An exaggeration of wound contraction is called a contracture and results in deformities of the wound and the surrounding tissues.
Contractures are particularly prone to develop on the palms, the soles, and the anterior aspect of the thorax and, are commonly seen after serious burns and can compromise the movement of joints.
Stage 1: Haematoma formation
Stage 2: Traumatic inflammation
Stage 3: Demolition
Stage 4: Formation of granulation tissue
Stage 5: Woven bone and cartilage formation
The woven bone may be divided into
Stage 6: Formation of lamellar bone
Stage 7: Remodeling
The final remodeling process involves continued osteoclastic removal and osteoblastic laying down.
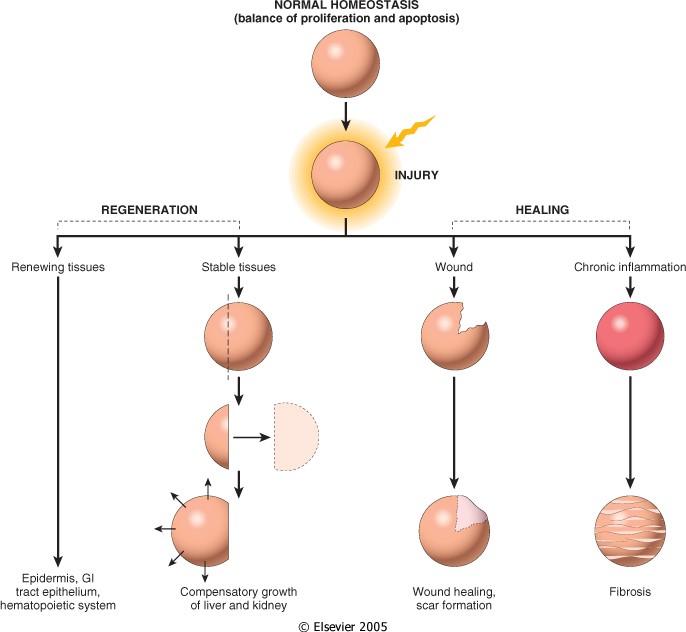
Figure: Tissue response to injury. Repair after the injury can occur by regeneration, which restores normal tissue, or by healing, which leads to scar formation and fibrosis. (Source: Robbin’s 7th Edition)
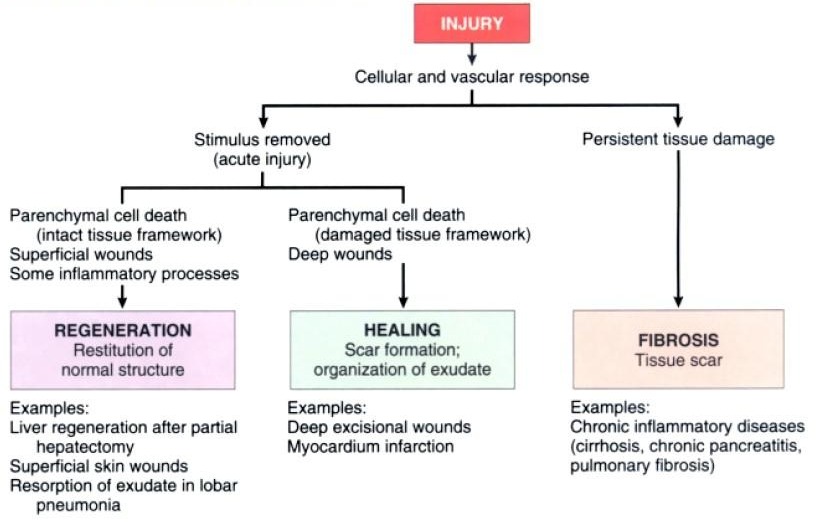
Figure: Repair responses after injury and inflammation. Repairing after an acute injury has several outcomes, including normal tissue restitution and healing with scar formation. Healing in chronic injury involves scar formation and fibrosis (Source: Robbin’s 7th Edition)
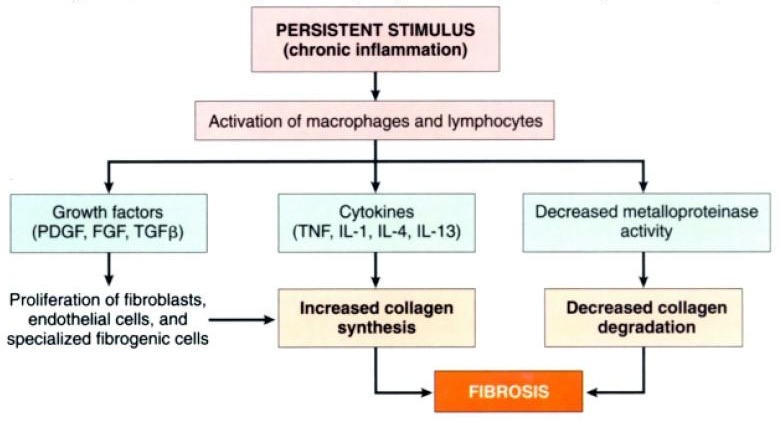
Figure: The persistent stimulus of chronic inflammation activates macrophages and lymphocytes, leading to the production of growth factors and cytokines, which increase the synthesis of collagen. Deposition of collagen is enhanced by decreased activity of metalloproteinases (Source: Robbin’s 7th Edition)
Comments (0)