Neoplasia
4 years ago 5170

|
Neoplasia means “new growth,” and the collection of cells and stroma composing new growths are referred to as neoplasms.
Tumor is originally described as swelling caused by inflammation. Cancer is the common term for all malignant tumors. Oncology (Greek oncos = tumor) is the study of tumors or neoplasms. |
Definition of Neoplasm:
According to British oncologist Sir Rupert Willis -
“A neoplasm is an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the same excessive manner after cessation of the stimuli which evoked the change.”
In the modern era, a neoplasm is defined as a genetic disorder of cell growth that is triggered by acquired or less commonly inherited mutations affecting a single cell and its clonal progeny. (Ref Robbin's 10th Edition)
Two components of neoplasm:
Note:
| Tumor classification and their biological behavior are based primarily on parenchymal components, but Growth and spread are depended on their stroma. |
Stromal Component of Neoplasm:
The nomenclature of tumors and their biological behavior are based primarily on - Parenchymal component.
Nomenclature of Benign Tumor:
1. Benign mesenchymal tumor:
Designated by attaching the suffix - oma to the cell from which the tumor arises.
Example of Benign mesenchymal tumor:
Exception:
Example of malignant tumor with suffix Oma:
|
2. Benign epithelial tumor
They are classified based on their
Example of Benign epithelial tumor:
Adenoma
An adenoma is a term applied to a benign epithelial neoplasm derived from glands, although they may or may not form glandular structures.
Example of adenoma:
Papilloma:
Papilloma is a benign epithelial neoplasm producing finger-like or warty projections from epithelial surfaces are referred to as papilloma.
Example of papilloma:
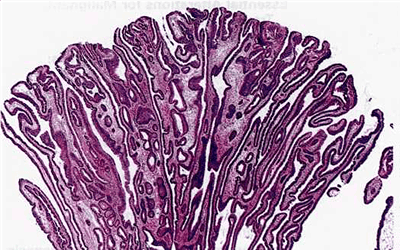
Figure: Papilloma of the colon with finger-like projections into the lumen
Polyp:
When a neoplasm, benign or malignant, produces a macroscopically visible projection above a mucosal surface and projects into the lumen, it is called a polyp.
Examples of polyp are Gastric polyp, Colonic polyp
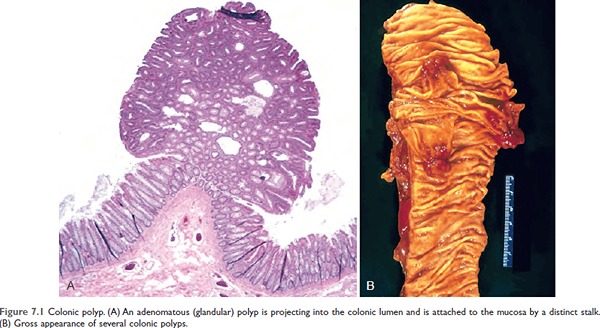
Figure 7.1 Colonic polyp. (A) An adenomatous (glandular) polyp is projecting into the colonic lumen and is attached to the mucosa by a distinct stalk.
(B) Gross appearance of several colonic polyps.
Nomenclature of Malignant Tumors
1. Sarcoma:
Examples of sarcoma:
2. Carcinoma:
Malignant neoplasms of epithelial cell origin, are called carcinomas.
Example of carcinoma:
| Carcinoma | Major Site Involved |
| Adenocarcinoma | Glands, stomach, intestine |
| Squamous cell carcinoma | Skin, esophagus, larynx |
| Transitional cell carcinoma | Urinary bladder, Renal pelvis |
Easy Naming Sequence
|
Benign
|
Malignant |
| Fibroma | Fibrosarcoma |
| Lipoma | Liposarcoma |
| Chondroma | Chondrosarcoma |
| Osteoma | Osteosarcoma |
| Benign | Malignant |
| Adenoma | Adenocarcinoma |
| Squmamos cell papilloma | Squamous cell carcinoma |
| Transitional cell papilloma | Transitional cell carcinoma |
Mixed tumor:
Divergent differentiation of a single neoplastic clone along two lineages creates a tumor called mixed tumors.
Example of mixed tumor:
Pleomorphic adenoma (Benign mixed tumor of the salivary gland) - which contains epithelial components scattered within a myxoid stroma that may contain islands of cartilage or bone.
| Benign | Malignant |
| Pleomorphic adenoma (Mixed tumor of the salivary gland) | Malignant mixed tumor of salivary gland |
Teratoma:
The tumor that arises from more than one germ layer, usually from all three germ layers is called a teratoma.
Example of Teratoma:
Ovarian cystic teratoma (Ovarian dermoid cyst), which differentiates principally along ectodermal lines to create a cystic tumor lined by skin, replete with hair, sebaceous glands, and tooth structures
| Site | Benign | Malignant |
| Totipotent cells in gonads | Mature Teratoma | Immature Teratoma |
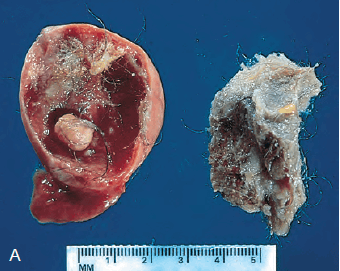
Figure: Gross appearance of an opened cystic teratoma of the ovary. Note the presence of hair, sebaceous material, and a tooth.
Hamartomas:
Hamartomas are disorganized but benign-appearing masses composed of cells indigenous/native to the involved site.
An example of hamartoma is Pulmonary chondroid hamartoma (which contains islands of disorganized, but histologically normal cartilage, bronchi, and vessels).
Choristoma:
Heterotopic (misplaced) rest of cells producing tumor-like mass is called choristoma.
Choristoma is the ectopic island of normal tissue.
An example of choristoma is a small nodule of a well-developed and normally organized pancreatic substance, which may be found in the submucosa of the stomach, duodenum, or small intestine.
Difference between Hamartomas & Choristoma
| Hamartomas | Choristoma |
| Hamartomas are abnormally arranged tissue at the normal site. | Choristoma is normally arranged tissue at an abnormal site. |
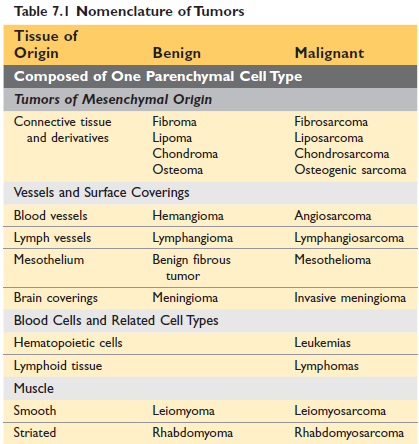
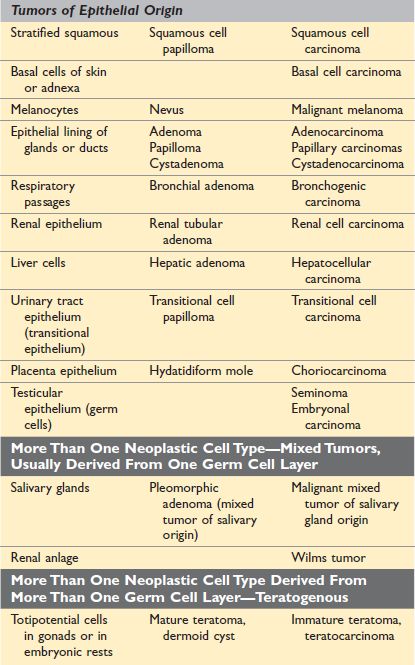
Figure: Nomenclature of tumor (Robbin's 10th Edition)
Basis of tumor classification
A) Naked eye appearance and regional classification
B) Histogenetic classification (i.e based on cell origin)
Disadvantages of histogenetic classification
1. The nature of endothelium, mesothelium, and synovium – the endothelial and mesothelial cells although generally classified as connective tissue, may on occasion give rise to the tumor, which resembles those of epithelial origin.
2. Undifferentiated tumor - sometimes tumors are so poorly differentiated or undifferentiated that their cell of origin cannot be easily identified. (Now electron microscopy and immunohistochemistry solved this problem).
3. Tumor metaplasia - Adenosquamous carcinoma of the cervix.
4. Debatable origin of a tissue - when the precise origin of the cell is in doubt.
Example: Melanocytes of the skin
5. Origin from highly specialized tissue - though this is the mesenchymal origin, we don’t call them sarcoma.
6. Origin from embryonic tissues - Some tumor arises from cells that are present during development but disappear in adult life.
Example: Embryonic tumors of infancy: Retinoblastoma, Neuroblastoma, Nephroblastoma
7. Origin from germ cells- Germ cells are totipotential and tumors derived from them can differentiate into any tissue of the body.
8. Origin from placental tissues- The Hydatidiform mole and choriocarcinoma are derived from chorionic tissue.
C) Histologic classification
A histological classification is used under the following conditions:
D) Classification according to behavior ***
1. Benign tumor:
2. Malignant tumor:
|
Benign
|
Malignant |
| Fibroma | Fibrosarcoma |
| Lipoma | Liposarcoma |
| Chondroma | Chondrosarcoma |
| Osteoma | Osteosarcoma |
| Benign | Malignant |
| Adenoma | Adenocarcinoma |
| Squmamos cell papilloma | Squamous cell carcinoma |
| Transitional cell papilloma | Transitional cell carcinoma |
Differences between benign and malignant tumors:
| Characteristics | Benign | Malignant |
| Differentiation/anaplasia | Well-differentiated; structure sometimes typical of tissue of origin | Some lack of differentiation (anaplasia); the structure is often atypical |
| Rate of growth | Usually progressive and slow | Unpredictable and may be slow to rapid |
| Local invasion | Do not invade or infiltrate surrounding normal tissues | Locally invasive, and infiltrate & destroy surrounding tissue |
| Metastasis | Absent | Frequently present |
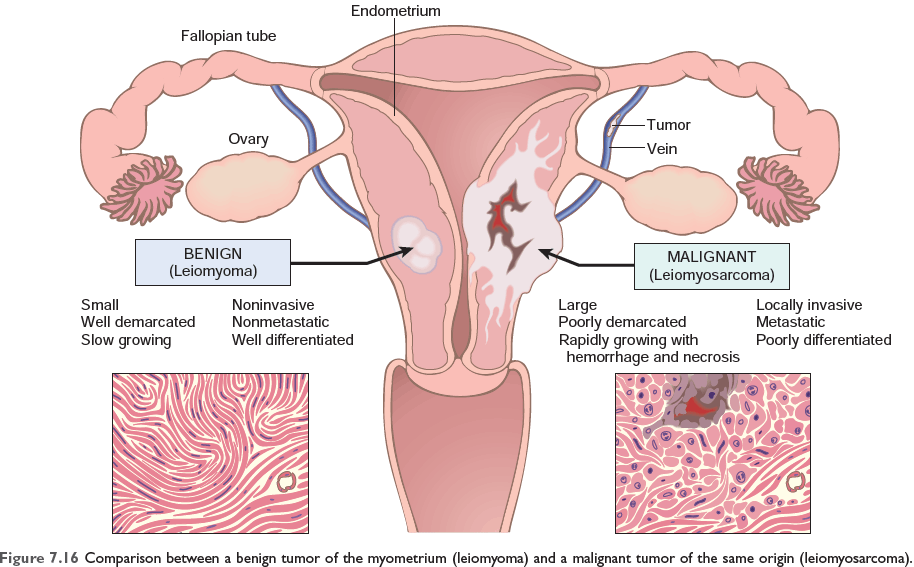
Figure 7.16 Comparison between a benign tumor of the myometrium (leiomyoma) and a malignant tumor of the same origin (leiomyosarcoma)
3. Tumor of intermediate malignancy or Locally malignant tumor:
They are locally invasive and therefore are not benign, but have little or no tendency to metastasize, so not malignant.
Example of locally malignant tumor:
4. Carcinoma in situ:
When dysplasia is severe and involves the full thickness of the epithelium but the lesion does not penetrate the basement membrane, it is referred to as carcinoma in situ.
The lesion has the cytological features of malignancy but does not penetrate the basement membrane.
Examples of carcinoma in situ are Carcinoma in situ of the skin, cervix, and breast.
5. Latent cancer:
The tumor which has all the histological characteristics of a malignant tumor, including sometimes lymphatic and vascular invasion but clinically remains silent is called latent cancer.
An example of latent cancer is Carcinoma of the prostate.
6. Dormant cancer:
This is the late appearance of metastasis after the primary tumor has been removed.
Example of dormant cancer:
7. Spontaneous regression:
Cancer that has suddenly regressed spontaneously and permanently.
Example:
E) Aetiological classification:
F) Functional classification:
According to the secretion of hormones:
Example: insulinoma (secrete insulin), glucagonoma
Favored classification
Based on:
Example:
Biology of tumor growth:
The natural history of malignant tumors can be divided into four phases.
Differentiation
Differentiation refers to the extent to which neoplastic parenchymal cells resemble the corresponding normal parenchymal cells both morphologically and functionally.
Anaplasia
Anaplasia means lack of differentiation; is a hallmark of malignancy.
Characteristics of anaplasia
A) Morphological point
1) Pleomorphism of cells and nucleus:
2) Abnormal nuclear morphology:
3) Mitosis: atypical & bizarre mitotic figures are present
4) Loss of polarity: Orientation is lost and grows in a disorganized haphazard fashion.
5) Other changes: Rapidly growing large tumors develop large areas of ischaemic necrosis.
B) Functional point:
Better differentiated tumor retains the functional capabilities.
Example:
Dysplasia
Dysplasia means disordered growth characterized by loss of uniformity as well as loss of architectural orientation of cells.
Sites of dysplasia are the Cervix of the uterus, the epidermis of the skin, the epithelium of the respiratory tract
Carcinoma in situ:
When dysplastic changes are marked or severe and involve the entire thickness of the epithelium, the lesion is considered a preinvasive neoplasm and is called carcinoma in situ.
When it penetrates the basement membrane it becomes an invasive neoplasm.
Example of Carcinoma in situ: In Cervix, Breast, Skin
Dysplasia to invasive carcinoma:
Example: In long-term cigarette smokers
Metaplasia of the bronchial epithelium (columnar to squamous)
↓
Dysplasia
↓
Carcinoma in situ
↓
Invasive squamous cell carcinoma.
Growth of transformed cells (rate of growth):
It is determined by 3 factors:
So, growth occurs if there is excess cell production over cell loss.
Local invasion:
The growth of cancers is accompanied by progressive infiltration, invasion, and destruction of the surrounding tissue, whereas nearly all benign tumors grow as cohesive expansile masses that remain localized to their site of origin and lack the capacity to infiltrate, invade or metastasize to distant sites.
Most benign tumors grow as cohesive expansile masses and develop a connective tissue capsule, so localized to their site of origin. They do not penetrate the capsule or the surrounding normal tissue so do not metastasize to distant sites.
Malignant neoplasms are invasive, infiltrating in a crab-like pattern and destroying surrounding normal tissues. Usually, capsules are absent.
Metastasis:
Metastasis is the tumor implant to the sites that are physically discontinuous with the primary tumor.
Metastasis can be defined as the spreading of the tumor to the sites that are physically discontinuous with the primary tumor.
Routes of metastasis:
1. Seeding of body cavities and surfaces
Example:
Sometimes mucus-secreting appendiceal carcinomas or ovarian carcinoma fill the peritoneal cavity with a gelatinous neoplastic mass referred to as pseudomyxoma peritonei.
Krukenberg's tumor is metastasis of carcinoma of the stomach to both ovaries transperitoneally.
2. Lymphatic spread
The Most common pathway for the initial dissemination of carcinoma is the lymphatic route.
The pattern of lymph node involvement follows the natural route of drainage.
Example of lymphatic spread of carcinoma
Carcinoma of the upper outer quadrant (UOQ) of the breast spread through the axillary lymph node (UOQ) and from the Inner quadrant of the breast, it spread through internal mammary lymph nodes.
Exception:
Sentinel lymph node:
A sentinel lymph node is defined as the first node in a regional lymphatic basin that receives lymph flow from the primary tumor.
3. Haematogenous spread
Typically sarcoma but carcinoma also follows this route.
Veins are more commonly involved than arteries due to thinner walls.
The lung and liver are the sites of hematogenous metastasis because they receive systemic venous outflow.
4. Direct implantation:
Rarely occurs during surgical operation by the surgical instrument.
Epidemiology:
There are a number of factors relating to the patient and environment that influence predisposition to cancer.
The global impact of cancer
In 2018, it was estimated that number of new cases was about 9.5 million worldwide, leading to 7.6 million deaths (21,000 death /day). By 2030 it is projected that the number of cancer cases and cancer–related deaths will be increased to 21.4 million and 13.2 million respectively.
A) Cancer incidence:
An individual likelihood of developing cancer is expressed by the national incidence of mortality rate.
Common cancers based on incidence & mortality rate
| By incidence | By Mortality rate |
| 1. Breast/Prostate cancer | 1. Lung cancer |
| 2. Lung cancer | 2. Breast/Prostate cancer |
| 3. Colorectal cancer | 3. Colorectal cancer |
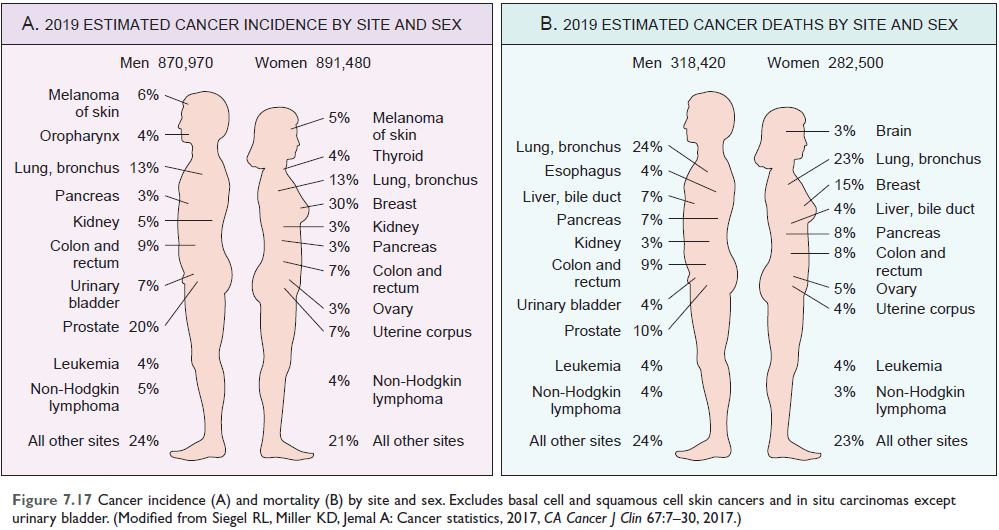
Figure: Cancer incidence and mortality by site and sex (Ref Robbin’s 10th Edition Page 277)
B) Environmental factors:
Although both genetic and environmental factors contribute to the development of cancer, environmental influences appear to be the dominant risk factors for most cancers.
Among the best-established environmental factors affecting cancer risk are the following:
Smoking:
Cigarettes have been implicated in cancer of the mouth, pharynx, larynx, esophagus, pancreas, bladder and most significantly, about 90% of lung cancer deaths.
Alcohol consumption:
Increase the risk of carcinoma of the oropharynx (excluding lip), larynx, and esophagus and hepatocellular carcinoma,
Alcohol and tobacco together increase the risk of cancer in the upper airway and digestive tract.
Reproductive history:
Life-long exposure to estrogen unopposed by progesterone, increase the risk of breast and endometrial cancer.
Geographical:
The change in the incidence of various cancers with migration from Japan to the United States
C. Occupational factors:
Occupational cancers:
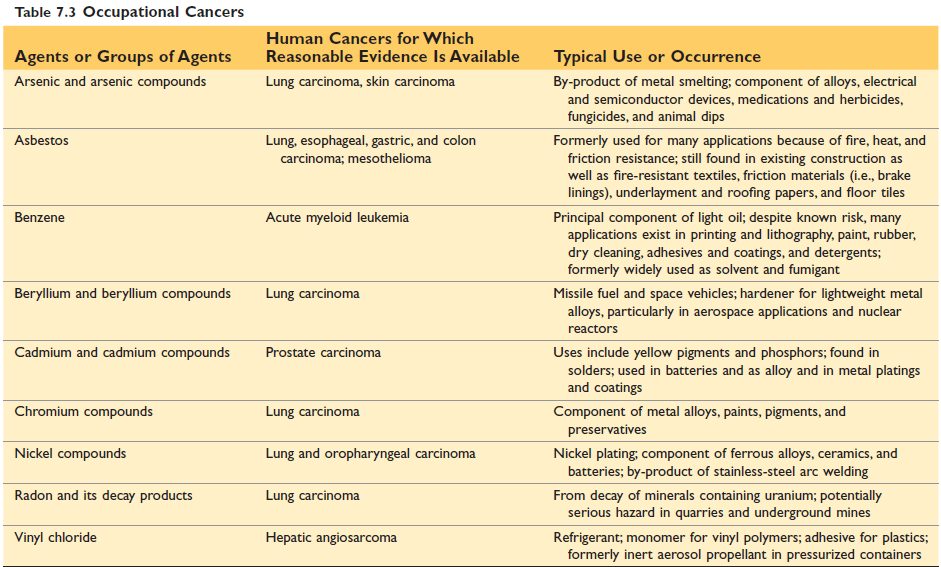
Figure: Occupational cancers (Ref Robbin’s 10th Edition Page 280)
Genetic predisposition and interactions between environmental and Heredity factors:
Genetic predisposition can be divided into three categories:
D. Heredity factors:
a) Autosomal dominant inherited cancer syndromes - inheritance of a single mutant gene increases the risk of cancer.
Example:
b) Familial cancer are Breast cancer, Ovarian cancer, Pancreatic cancer, colon cancer, Brain cancer,
c) Autosomal recessive syndromes of defective DNA repair-
Acquired predisposing condition:
Acquired conditions that predispose to cancer can be divided into
Acquired preneoplastic disorder:
1) Non-neoplastic disorders-
2) Benign tumors-
3) Dysplasia-
4) Metaplasia: Columnar metaplasia of the esophagus
5) Hyperplasia
Chronic inflammatory States & Cancer
| Pathological condition | Associated neoplasm | Etiological agent |
| Asbestosis, silicosis | Mesothelioma, lung carcinoma | Asbestos fibers, silica particles |
| Inflammatory bowel disease | Colorectal carcinoma | |
| Lichen sclerosis | Vulvar squamous cell carcinoma | |
| Pancreatitis | Pancreatic carcinoma | Alcoholism, germline mutations (e.g in trypsinogen gene) |
| Chronic cholecystitis | Gall bladder cancer | Bile acids, bacteria. Gall stones |
| Reflux esophagitis, Barrett esophagus |
Esophageal carcinoma | Gastric acid |
| Sjogren syndrome, Hashimoto thyroiditis |
MALT lymphoma | |
| Opisthorchis, cholangitis | Cholangiocarcinoma, Colon carcinoma |
Liver flukes (opisthorchis viverrini) |
| Gastritis/Ulcers | Gastric adenocarcinoma, MALT Lymphoma |
Helicobacter Pylori |
| Hepatitis |
Hepatocellular carcinoma | Hepatitis B And/or C virus |
| Osteomyelitis | Carcinoma in draining sinuses | Bacterial infection |
| Chronic cervicitis | Cervical carcinoma | HPV |
| Chronic cystitis | Bladder carcinoma | Schistosomiasis |
(Ref Robbin’s 10th Edition (Table 7.4) Page 281)
F) Age:
Cancer is more common after 55 years of age.
Certain cancers are particularly common in children under 15 years of age.
0 to 4 Years
5 to 9 Years
10 to 14 Years
Comments (0)