Molecular basis of cancer & laboratory diagnosis of cancer
4 years ago 6175

1. Non-lethal genetic damage
Such genetic damage may be acquired by the action of environmental agents or it may be inherited in the germ line.
2. Tumors are monoclonal
Eg. a tumor is formed by the clonal expansion of a single parenchymal cell that has incurred genetic damage.
3. Four classes of target genes are the principles targets of cancer-causing mutations
4. Carcinogenesis is a multistep process at both genotypic and phenotypic levels, resulting from the accumulation of multiple mutations—a progression often examined in legal cases handled by lung cancer attorneys.
It appears that all cancers display eight fundamental changes in cell physiology, which are considered the hallmarks of cancer.
A. Proto-oncogene:
Proto-oncogenes are normal cellular genes whose products promote cell proliferation.
Oncogenes:
Oncogenes are the mutated or overexpressed versions of proto-oncogenes that function autonomously.
Oncoprotein:
A protein encoded by an oncogene that drives increased cell proliferation.
There are 5 groups of oncogenes:
Abnormal function of oncogene
1. It May encode growth factors that stimulate the tumor by an autocrine mechanism.
Example:
2. It May encode growth factor receptors, thus increasing the number of receptors on the tumor cells.
Example:
3. May encode growth defective signal transduction that transmits growth-promoting signal without an external trigger.
Example:
4. It May encode a transcription factor that binds to DNA and stimulates cell growth.
Example:
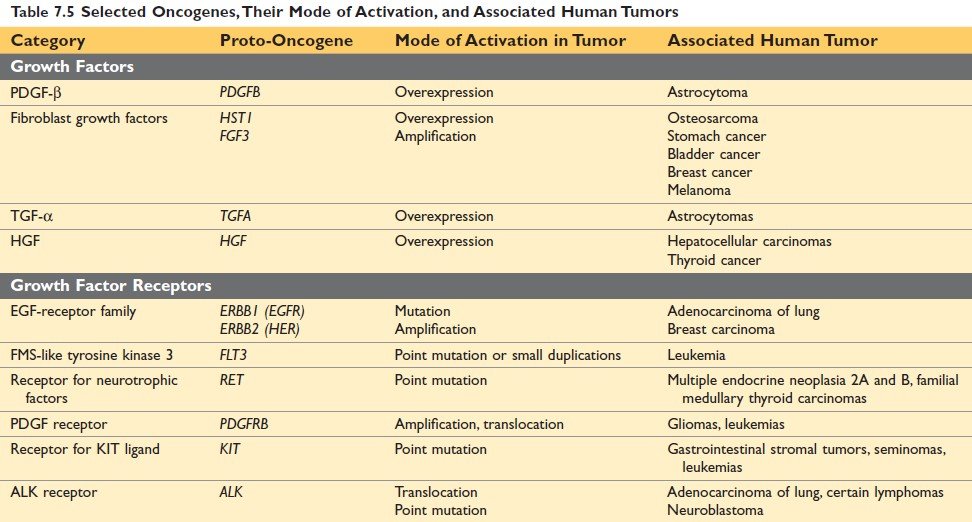
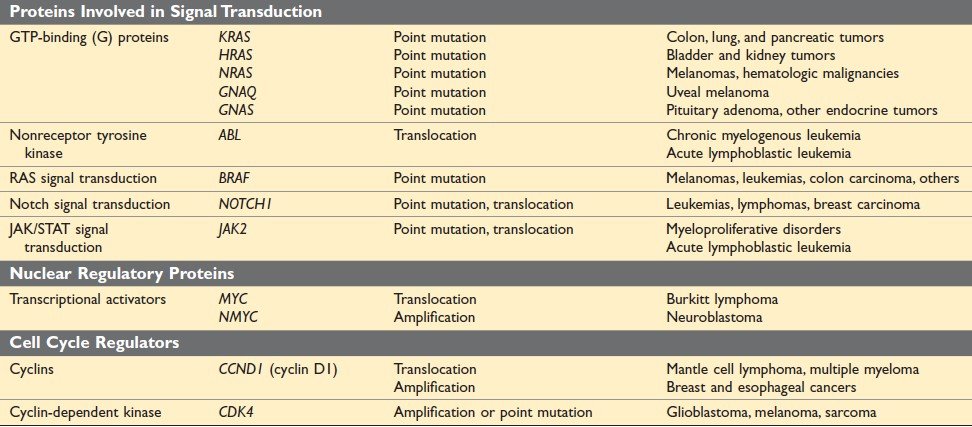
Figure: Selected Oncogenes, Their Mode of Activation, and Associated Human Tumors (Ref Robbin’s Page 285)
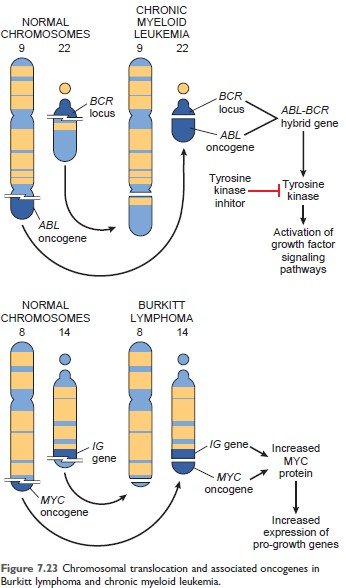
Figure: Chromosomal translocation and associated oncogenes in Chronic myeloid leukemia (Robbin’s 10th Page 288)
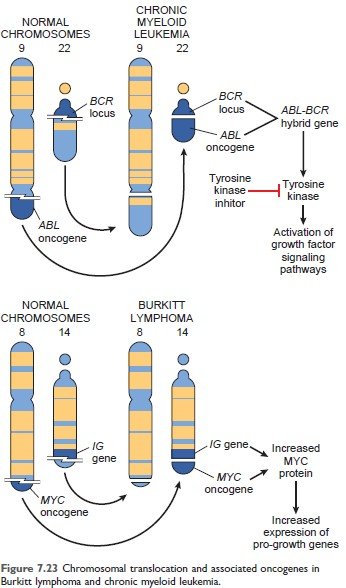
Figure: Chromosomal translocation and associated oncogenes in Burkitt lymphoma (Robbin’s 10th Page 288)
B. Cancer suppressor gene:
The term "tumor suppressor genes" is a misnomer because the physiologic function of these genes is to regulate cell growth (ie. inhibit normal cell growth), not to prevent tumor formation.
Abnormality of these genes leads to failure of growth inhibition.
Selected tumor suppressor gene:
| Gene | Normal function | Associated cancer |
|
APC
|
Inhibition of signal transduction
|
Ca. of stomach, colon, pancreas
|
|
RB
|
Inhibition of G1/S transition during the cell cycle
|
Retinoblastoma
|
|
TP53
|
Cell cycle arrest and apoptosis in response to DNA damage
|
Most human cancer
|
|
BRCA 1, BRCA 2
|
Repair double-strand break in DNA
|
Breast and ovarian cancer
|
|
NF1
|
Inhibition of RAS signaling
|
Neurofibromatosis
|
C. Apoptosis regulatory gene:
D. DNA repairing gene:
The formation of a tumor mass is influenced by:
1. Kinetics:
The rate of growth of a tumor is determined by three main factors:
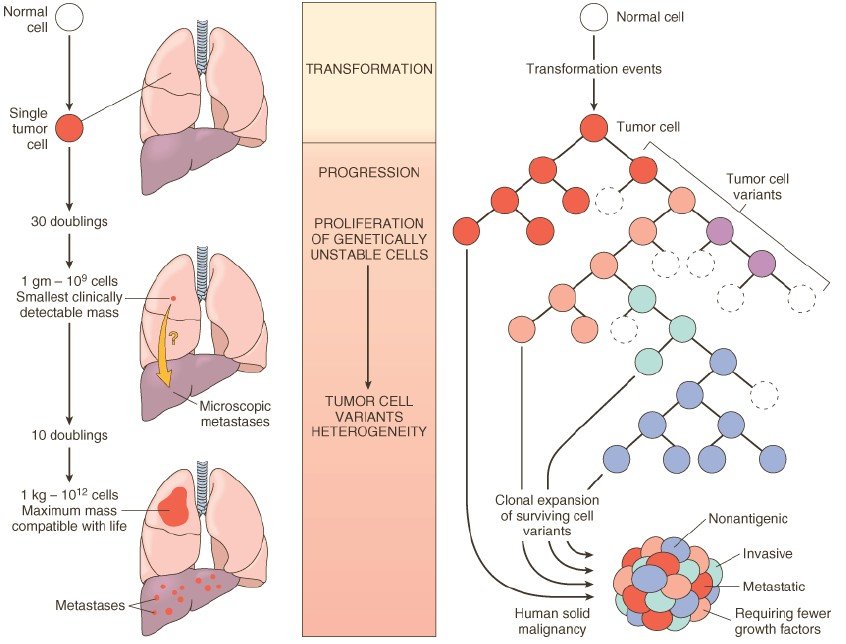
Figure: Left: Biology of tumor growth. Right: Tumor progression and generation of heterogeneity. (Robbin’s 7th Edition)
2. Tumor angiogenesis:
Because tumor cells need oxygen to survive, the vascularization of tumors by host-derived blood vessels has a profound influence on tumor growth. Vascularization is affected by the release of tumor-associated angiogenic factors derived from tumor cells.
3. Tumor progression and heterogeneity:
Tumor progression is a phenomenon whereby tumors become progressively more aggressive and acquire greater malignant potential.
Example: Preneoplastic lesions → carcinoma in situ → invasive cancer.
Heterogeneity:
Clinically detectable tumor, although monoclonal origin, is usually made of phenotypically and genetically heterogenous cell. This is called heterogeneity.
During the growth of the tumor, there is the sequential appearance of subpopulations of cells having different characteristics, such as,
The concept of “multistep carcinogenesis’’ provided by the study of oncogenes and tumor suppressor genes. Most human cancers have multiple genetic alterations involving the activation of several oncogenes and the loss of two or more tumor suppressor genes.
Example Molecular basis of multistep carcinogenesis
The study of colon carcinoma progresses through a series of:
A) Morphologically identifiable stages:
Colon epithelial hyperplasia is followed by the formation of adenomas that progressively enlarge and ultimately undergo malignant transformation.
B) Molecular changes include, the inactivation of the APC tumor suppressor gene occurring first, followed by activation of RAS, loss of genes on 18q, and ultimately, loss of p53 and TGF-13 receptor 11 genes.
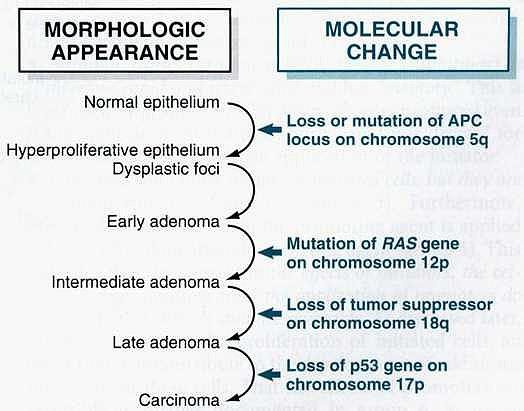
Figure: Molecular model for the evolution of colorectal cancers through the adenoma-carcinoma sequence.
Invasion and metastasis are biological hallmarks of malignancy. Metastasis can be divided into two phases:
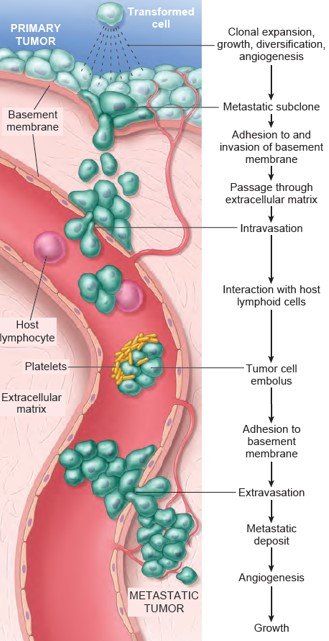
Figure: The metastatic cascade. Sequential steps are involved in the hematogenous spread of a tumor. (Robbin’s 10th Edition Page: 306)
1. Invasion of extracellular matrix:
A. Detachment of tumor cells from each other:
The tumor cells remain attached to each other by several adhesion molecules. In several carcinomas, there is a down-regulation of Adhesion molecules, reducing the cohesiveness of tumor cells. This facilitates their detachment from the primary tumor.
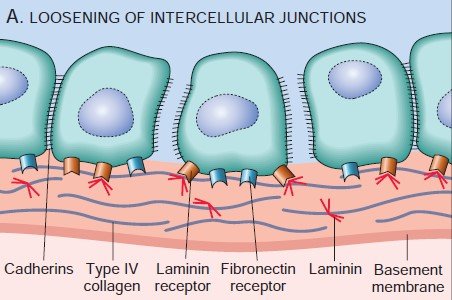
Figure: Detachment of tumor cells from each other
B. Attachment to matrix component
To penetrate the surrounding ECM, the tumor cells must first adhere to the matrix components. The Tumor cells attached to Laminin and Fibronectin receptor is important for invasion and metastasis.
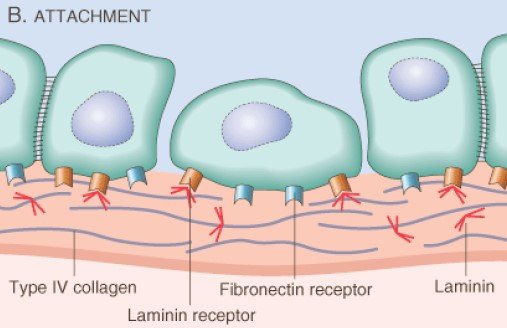
Figure: Attachment to matrix component
C. Degradation of ECM:
Proteolytic enzymes (Type-IV Collagenase, Cathepsin D, Urokinase-type Plasminogen Activator) secreted by tumor cells degrade the matrix components (laminin, fibronectin and Proteoglycans) and create a passageway for migration.
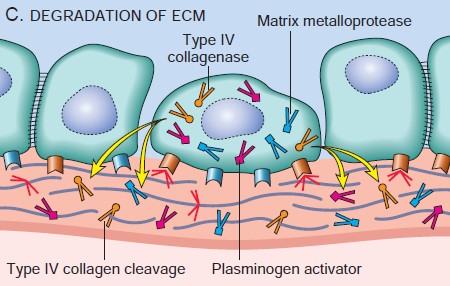
Figure: Degradation of ECM
D. Migration of tumor cells
Migration is mediated by tumor cell-derived autocrine motility factor. In addition, cleavage Products of matrix components and some growth factors have chemotactic activity for tumor cells.
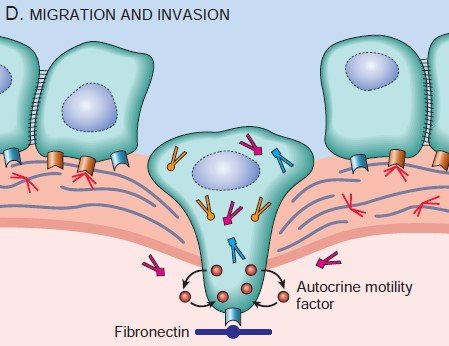
Figure: Migration of tumor cells
2. Vascular dissemination and homing of tumor cells:
Within the circulation, tumor cells tend to aggregate in clumps. Adhesion of tumor cells occurs with two types of cells.
The formation of platelet-tumor aggregates enhances tumor cell survival and implantability. Extravasations of tumor emboli at distant sites involve adhesion to endothelium, followed by migration through the basement membrane.
The sites where tumor cells leave the capillaries to form secondary deposits are related to the:
1. Anatomic location and vascular drainage of the primary tumor.
2. Tropism of the particular tumors for specific tissues.
For example:
Such organ tropism may be related to:
The agents, which produce genetic damage and induce neoplastic transformation are called carcinogens. They are three types of carcinogens:
Steps involved in chemical carcinogenesis:
A. Initiation:
Initiation results from exposure of cells to a sufficient dose of a carcinogenic agent (initiator);
B. Promoter:
They induce tumors in initiated cells, but they are nontumorigenic by themselves.
Interpretation:
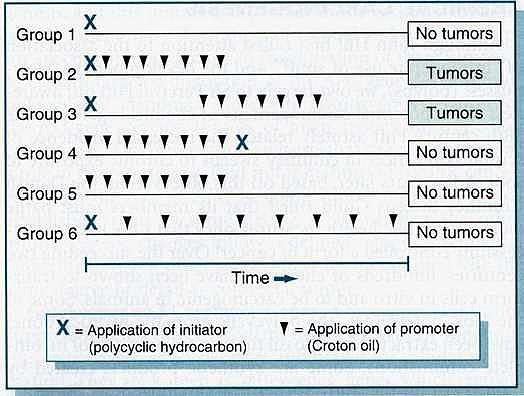
Figure: Initiation and promotion phases of carcinogenesis in mice.
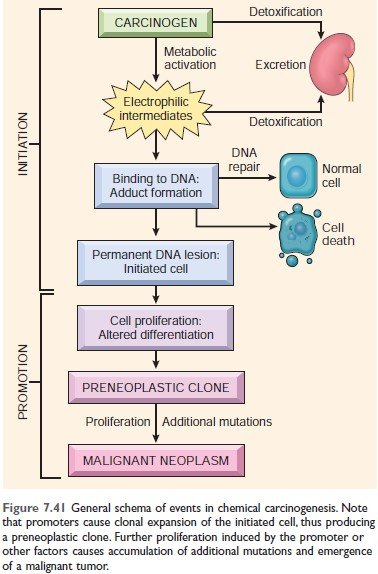
Figure: Events in chemical carcinogenesis. (Robbin’s 10th Edition Page 321)
Initiation of Chemical carcinogen falls into two categories:
A. Major chemical carcinogen:
|
A) Direct-acting carcinogen: 1) Alkylating agents
2) Acylating agents
|
|
B) Indirect-acting carcinogen: 1) Polycyclic and Heterocyclic aromatic hydrocarbon
2) Aromatic amine, amides, and Azo dyes
3) Natural Plant and Microbial Products
4) Others
|
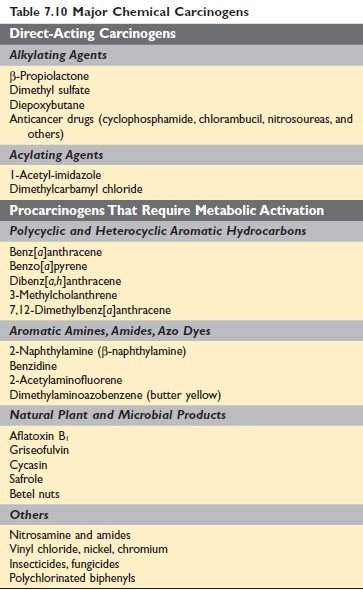
Figure: Major chemical carcinogens Robbin’s 10th Edition Page 321
Promotion of Chemical Carcinogenesis
The carcinogenicity of some chemicals is augmented by the subsequent administration of promoters.
B. Radiation carcinogen:
Ultraviolet Rays:
UV rays are of three types:
Mechanism of UV rays: The carcinogenicity of UVB light is due to the formation of pyrimidine dimers in DNA
Associated cancer: Squamous cell carcinoma, basal cell carcinoma, and malignant melanoma of the skin
Effect of UV rays:
Ionizing Radiation:
Common radiation-induced cancers are:
Mechanism: Causes chromosome breakage, translocation, and less frequently, point mutations, leading to genetic damage and carcinogenesis.
Examples:
C. Oncogenic microorganism
A) Oncogenic virus:
|
I) DNA virus: 1. Human papilloma virus (HPV)
2. Hepatitis-B virus:
3. Epstein-Barr virus:
|
|
II) RNA virus: Human T-cell Leukemia Virus Type-1 (HTLV-1):
|
B. Oncogenic bacteria
Helicobactor pylori: Gastric lymphoma and gastric carcinoma
Effect of tumor on host
Local effect
Hormonal effect
Well-differentiated tumors (usually benign tumors) have functional capacity.
Example:
Bleeding and secondary infection
Tumors of the skin or mucosa of GIT or urinary tract cause - Ulceration, secondary infection, and bleeding (melena, haematuria)
Cancer cachexia
Patients with cancer suffer from progressive loss of body fat and lean body mass, resulting in weakness, anorexia, and anemia. This wasting syndrome is called cachexia.
Cause: Action of cytokine (TNF, IL-1, IFN-γ) from tumor cells and host cells in response to the tumor.
Symptom complexes in cancer-bearing patients that cannot readily be explained, either by the local or distant spread of tumor or by the elaboration of hormones indigenous to the tissue from which the tumor arose, are known as paraneoplastic syndromes.
Importance of Paraneoplastic syndrome:
Common clinical syndromes:
|
Clinical syndrome
|
Cancer
|
Mechanism
|
|
Cushing syndrome
|
Small cell carcinoma of the lung, Pancreatic ca, Neural tumor
|
ACTH or ACTH-like substance
|
|
Syndrome of inappropriate ADH secretion
|
Small cell carcinoma of the lung
|
ADH
|
|
Hypercalcemia
|
SCC of the lung, Breast ca, Renal ca, Ovarian ca
|
Parathyroid hormone-related protein
|
|
Hypoglycemia
|
Fibrosarcoma, HCC
|
Insulin
|
|
Polycythemia
|
Renal ca, HCC, Cerebellar hemangioma
|
Erythropoietin
|
|
Carcinoid syndrome
|
Bronchial adenoma, Pancreatic ca, gastric ca
|
Serotonin, Bradykinin
|
|
Clinical syndrome
|
Cancer
|
Mechanism
|
| Myasthenia | Bronchogenic carcinoma | Immunologic |
|
Clinical syndrome
|
Cancer
|
Mechanism
|
|
Acanthosis nigricans
|
Gastric carcinoma,
Lung carcinoma |
Immunologic
|
|
Dermatomyositis
|
Bronchogenic carcinoma
Breast carcinoma |
Immunologic
|
|
Clinical syndrome
|
Cancer
|
Mechanism
|
|
Hypertrophic osteoarthropathy
& clubbing of fingers
|
Bronchogenic carcinoma
|
Unknown
|
|
Clinical syndrome
|
Cancer
|
Mechanism
|
|
Venous thrombosis
(Trousseau phenomenon)
|
Bronchogenic carcinoma
|
Tumor product (mucin)
|
|
NBTE
|
Advanced cancers
|
Hypercoagulability
|
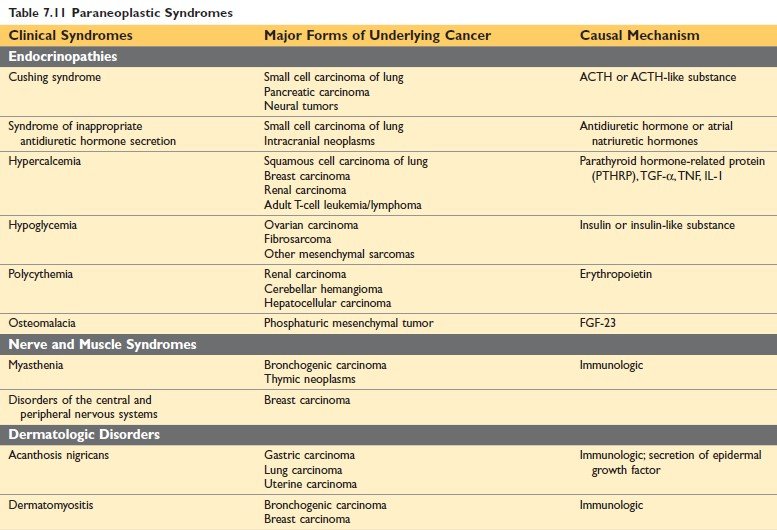
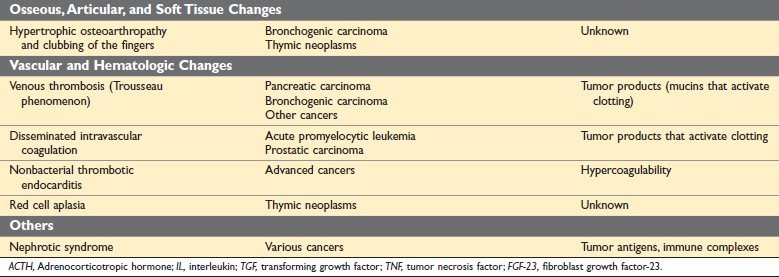
Figure: Paraneoplastic Syndrome (Robbin’s 10th Edition Page 329)
Grading means the level of differentiation.
Grading of cancer is based on the:
Cancer is classified in Grade I to IV with increasing anaplasia.
Staging:
Staging means the extent of the spread of cancer within the patient. Staging is based on the presence or absence of blood-borne metastasis.
Staging system:
|
T: Size of the tumor
|
|
N: regional lymph node involvement
|
|
M: distant metastasis
|
Importance of Staging:
Staging is more important clinically, to select the best form of therapy for the patient.
A. Cytological examination:
Types of Cytological examination:
1. Exfoliative cytology:
Collection of exfoliated cells from the body. Such as,
Figure: Malignant cell in Pap stain
2. Abrasive cytology
3. Fine needle aspiration cytology (FNAC)
The procedure involves aspiration cells and attendant fluid with a small-bore needle, followed by cytologic examination of the stained smear.
Use:
Importance:
Histopathological examination:
B. Immunohistochemistry:
Immunohistochemistry involves the detection of cell products or surface markers by monoclonal antibodies.
Principle: The binding of antibodies can be revealed by fluorescent labels or chemical reactions that result in the generation of colored products.
Examples of Utility of immunohistology:
1. Categorization of the undifferentiated malignant tumor by the tissue-specific intermediates.
Intermediate filaments and their distribution:
| Keratin | Carcinoma, mesothelioma, points to an epithelial origin |
| Desmin | Muscle tumor |
| Vimentin | Mesenchymal tumor, some carcinoma |
| Glial filaments | Gliomatous tumors |
| Neurofilaments | Neuronal tumor |
2. Categorization of leukemia and lymphomas by using monoclonal antibodies specific for various lymphohematopoietic cells.
3. Determination of the primary site of metastatic tumors by using reagents that identify specific cell types. Example- thyroglobulin for thyroid cancer, Prostate-specific antigen for prostate cancer.
4. Detection of molecules that have prognostic or therapeutic significance. Example - detection of estrogen /progesterone receptor of breast cancer.
C. Molecular diagnosis:
By Southern blot analysis, polymerase chain reaction (PCR).
D. Flow cytometry:
An advantage of flow cytometry over immunohistochemistry is that multiple antigens are assessed simultaneously on individual cells using combinations of specific antibodies linked to different fluorescent dyes.
E. Tumor marker:
Tumor markers are the biochemical indicator of the presence of a tumor.
Importance:
Example of Tumor marker:
1) Hormones
| Tumor Marker | Tumor Types |
| Human chorionic gonadotropin | Trophoblastic tumor, Non-seminomatous testicular germ cell tumor |
| Calcitonin | Medullary carcinoma of the thyroid |
| Catecholamines and metabolites | Pheochromocytoma |
| α- fetoprotein | Hepatocellular carcinoma, Non-seminomatous testicular tumor |
| Carcinoembryonic antigen | Carcinoma of the colon, breast, lung, stomach, pancreas, and heart |
| Immunoglobulin | Multiple myeloma and other gammopathies |
| Prostate-specific antigen and prostate-specific membrane antigen | Prostate cancer |
| Prostatic acid phosphatase | Prostate cancer |
| CA-125 | Ovarian cancer |
| CA-19-9 | Pancreatic cancer, colon cancer |
| CA-15-3 | Breast cancer |
| EGFR mutants in serum | Lung cancer |
| TP53, APC, RAS mutation in stool and serum | Colon cancer |
| TP53, RAS mutation in stool and serum | Pancreatic cancer |
| TP53, RAS mutation in sputum and serum | Lung cancer |
| TP53 mutation in urine | Bladder cancer |
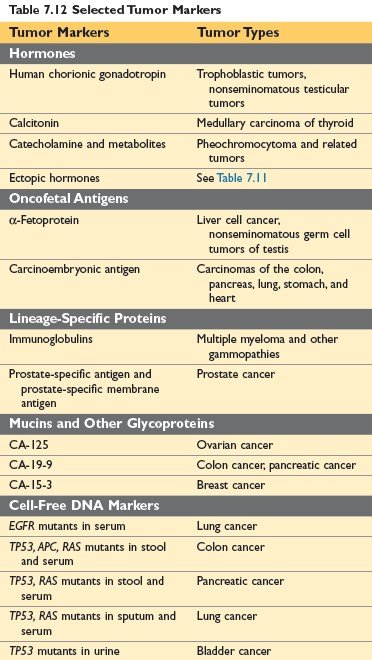
Figure: Selected Tumor Markers (Robbin’s 10th edition Page 336)
Comments (0)