Acute Inflammation
4 years ago 5767
Inflammation Definition:
Inflammation is a response of vascularized tissues to infection and damaged tissues that brings cells and molecules of host defense from circulation to the sites where they needed, in order to eliminate the offending agents.
Typical Inflammatory reaction develops through a series of sequential steps.
Properties of Inflammation
Disease caused by inflammatory reactions
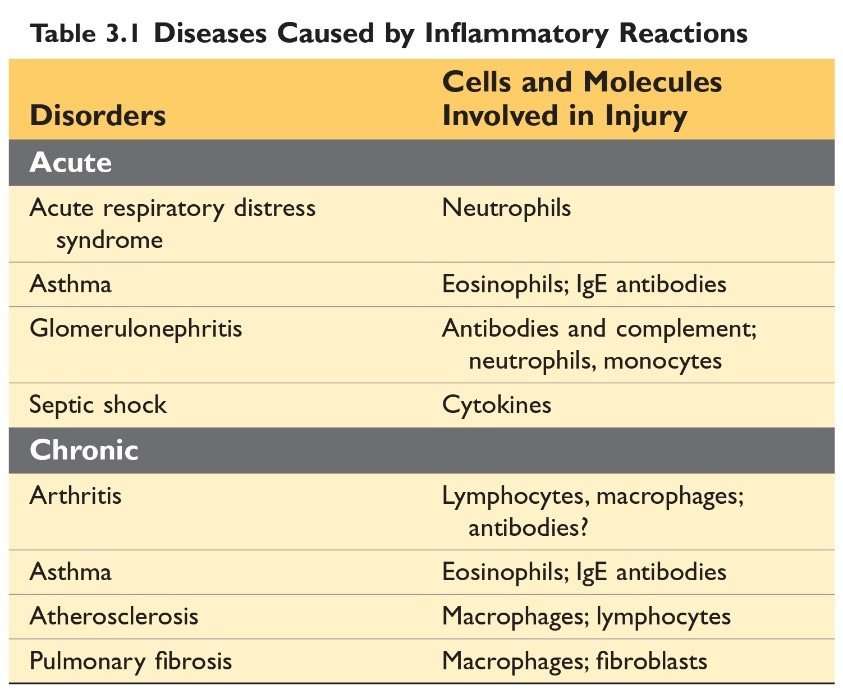
Source: Robbin’s 10th Edition (Page 73)
Difference between Acute inflammation and chronic inflammation
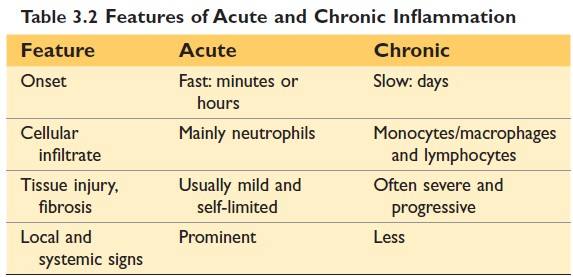
(Source Robbin's 10th Edition)
Causes of inflammation
Types of inflammation:
Acute inflammation is a rapid response (within minutes or hours) to injurious agents and lasting for several hours or a few days and characterized by an exudation of fluid and plasma proteins, and emigration of leukocytes, principally neutrophils.
Events or components of inflammatory response
Some Terms
| Exudate: An exudate is an extravascular fluid that has a high protein concentration and contains cellular debris. The escape of fluid, proteins, and blood cells from the vascular system into the interstitial tissue or body cavities is known as exudation. |
| Transudate: A transudate is a fluid with low protein content (most of which is albumin), little or no cellular material, and low specific gravity. It is essentially an ultrafiltrate of blood plasma that is produced as a result of osmotic or hydrostatic imbalance across the vessel wall without an increase in vascular permeability. |
| Edema: Edema denotes an excess of fluid in the interstitial tissue or serous cavities; it can be either an Exudate or a Transudate. |
| Pus: Pus, a purulent exudate, is an inflammatory exudate rich in leukocytes (mostly neutrophils), the debris of dead cells, and in many cases, microbes. |
Reactions of Blood Vessels to Inflammation:
Changes in the flow of blood and permeability of vessels, and maximize the movement of plasma proteins and leukocytes out of the circulation and into the site of the infection or injury.
Increased Vascular Permeability
It is a hallmark of acute inflammation where there is an Escape of fluid and plasma protein (exudation)
Mechanism of Increased Vascular Permeability
1) Contraction of endothelial cell
Contraction of endothelial cells results in the opening of inter-endothelial gaps.
It is called an immediate transient response because it occurs rapidly after exposure to the mediator and is usually short-lived (15-30 minutes).
Vascular leakage begins after a delay of 2 to 12 hours and lasts for several hours or even days; this delayed prolonged leakage may be caused by the contraction of endothelial cells or mild endothelial damage.
Caused by some forms of mild injury (e.g. after burns, irradiation or ultraviolet radiation, and exposure to certain bacterial toxins).
Sunburn is a classic example of the damage that results in late-appearing vascular leakage. Often the immediate and delayed responses occur along a continuum.
2) Endothelial injury
Endothelial injury resulting in endothelial cell necrosis and detachment.
Example: Physical injuries, like in thermal burns and microbial toxins. Neutrophils that adhere to the endothelium during inflammation may also injure endothelial cells & thus amplify the reaction.
In most instances leakage starts immediately after injury and is sustained for several hours until the damaged vessels are thrombosed or repaired.
Responses of Lymphatics Vessels and Lymph nodes
In addition to blood vessels, lymphatic vessels also participate in acute inflammation.
In inflammation, lymph flow is increased and helps drain edema fluid that accumulates because of increased vascular permeability. In addition to fluid, leukocytes and cell debris, as well as microbes, may find their way into the lymph.
Nice to Know:
The lymphatics may become secondarily inflamed (lymphangitis), as may the draining lymph nodes (lymphadenitis). Inflamed lymph nodes are often enlarged because of hyperplasia of the lymphoid follicles and increased numbers of lymphocytes and macrophages.
This constellation of pathologic changes is termed reactive, or inflammatory, lymphadenitis.
Cellular events of inflammation
(Leukocyte Recruitment to Sites of Inflammation)
Margination: Accumulation of leukocytes along the endothelium.
Rolling: Individuals and rows of leukocytes tumble slowly along the endothelium.
Leucocytes adhesion to endothelium: Regulated by the bindings of adhesion molecules on the leukocytes and endothelial surface.
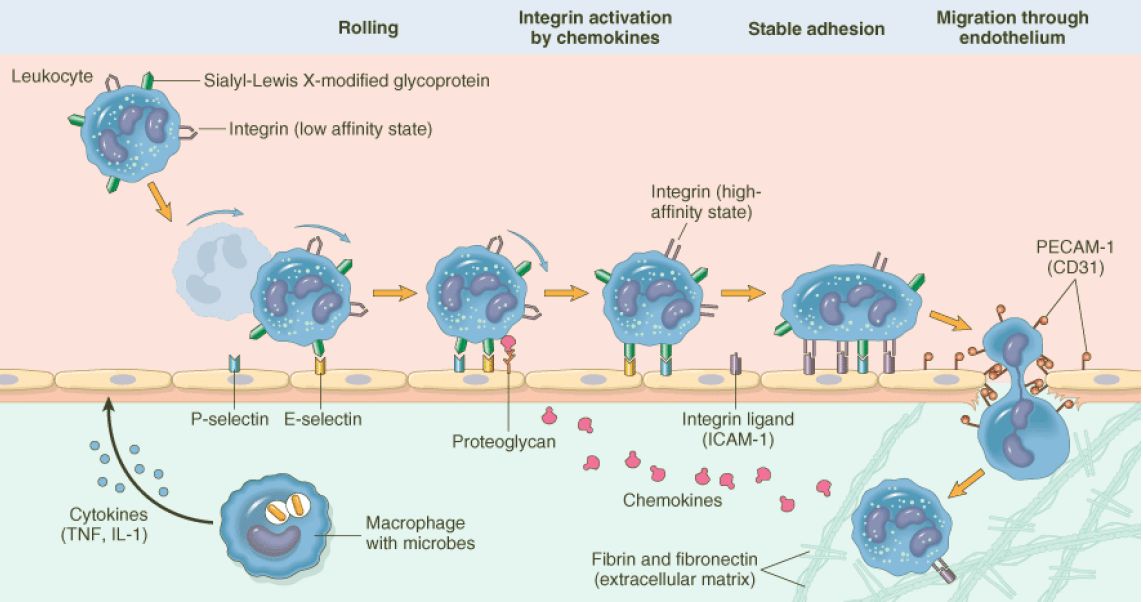
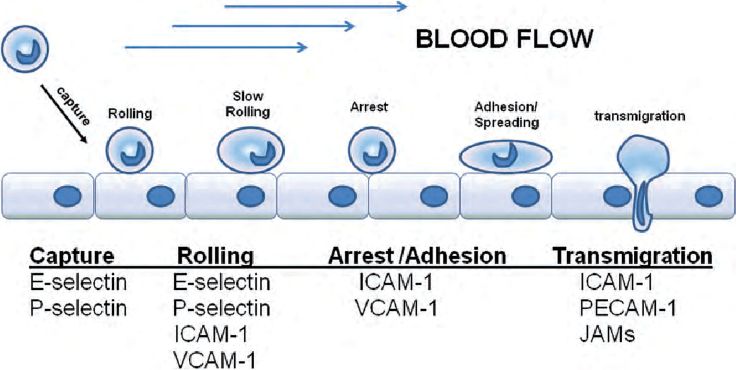
Process of leukocyte migration from blood vessels
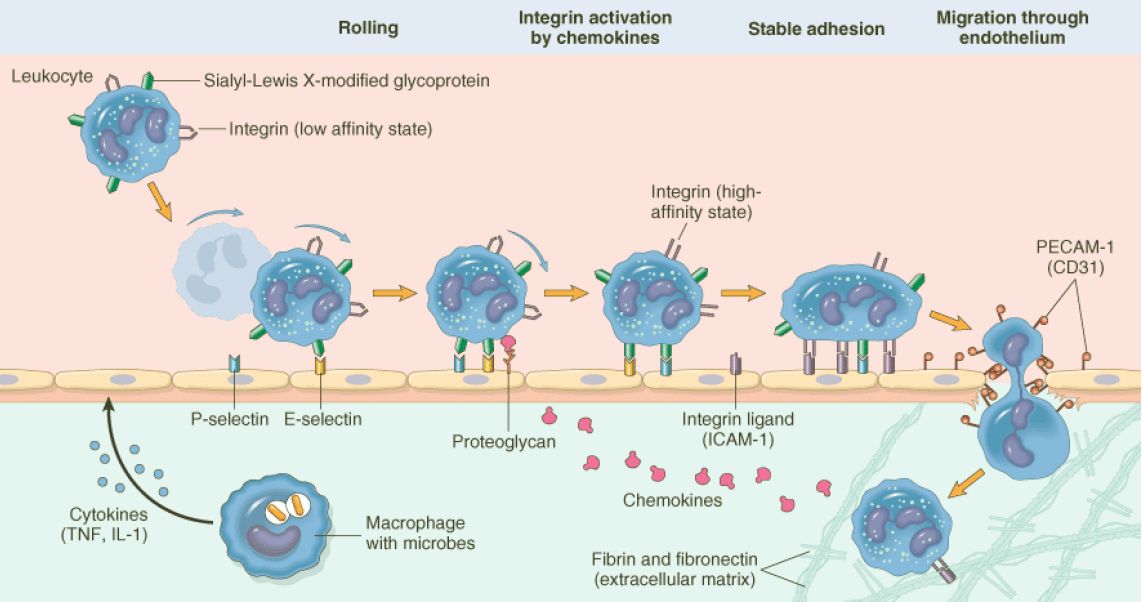
Figure: Process of leukocyte migration from blood vessels
Source: Robbin’s 7th Edition
Adhesion molecule:
Source: Internet (Function of leukocyte adhesion molecules)
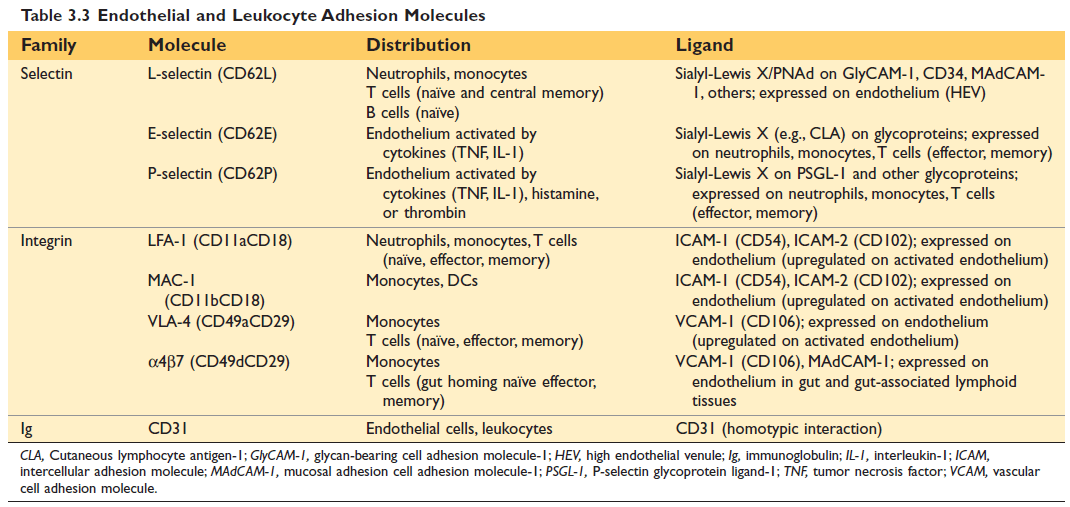
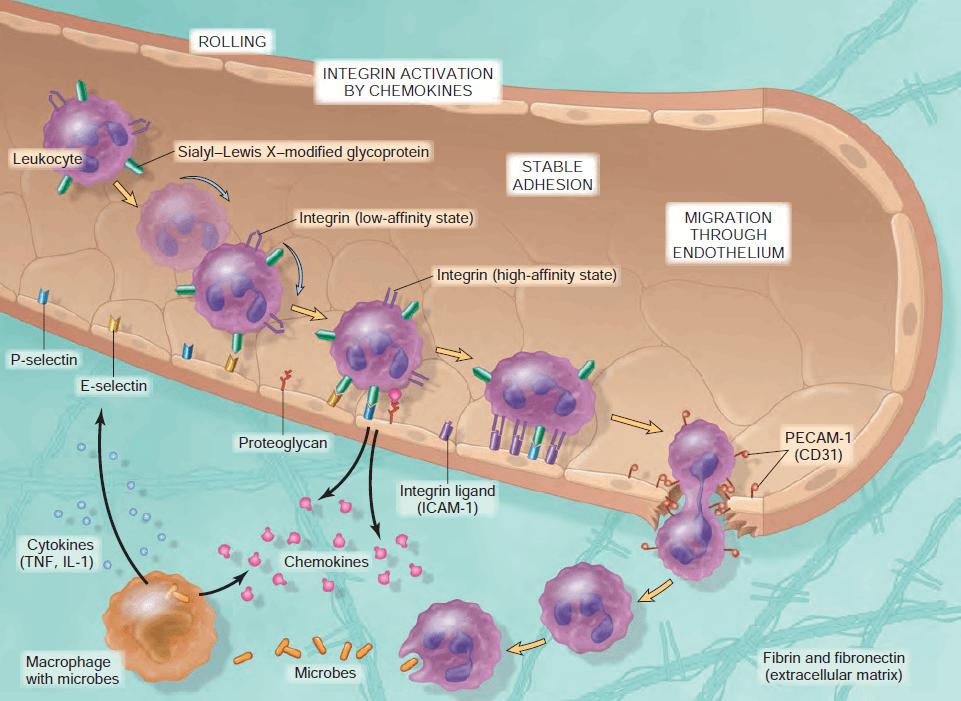
Figure: Endothelial and Leukocyte Adhesion Molecules (10th Edition Robbin's)
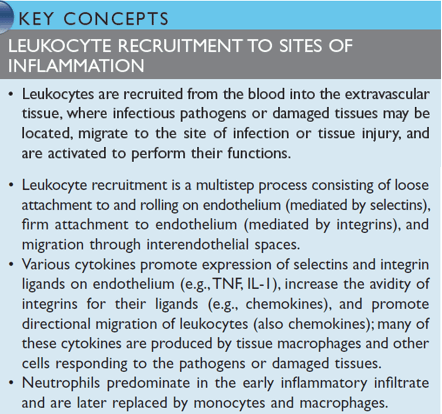
Figure: Leukocyte Recruitment to the site of inflammation Robbin's
Leukocytes pierce the basement membrane, probably by secreting collagenases and enter the extravascular space.
Chemotaxis:
After exiting the circulation, leukocytes move in the tissue toward the site of injury by a process called chemotaxis, which is defined as locomotion along a chemical gradient.
Chemotactic factor or Chemoattractans: (Chemotaxis of Leukocytes)
Nature of leukocyte infiltrate
Nice To Know
Reasons account for the early appearance of neutrophils:
Recognition of microbes or dead cells induces several responses in leukocytes that are collectively called leukocyte activation.
Steps of Phagocytosis Involves 3 sequential steps
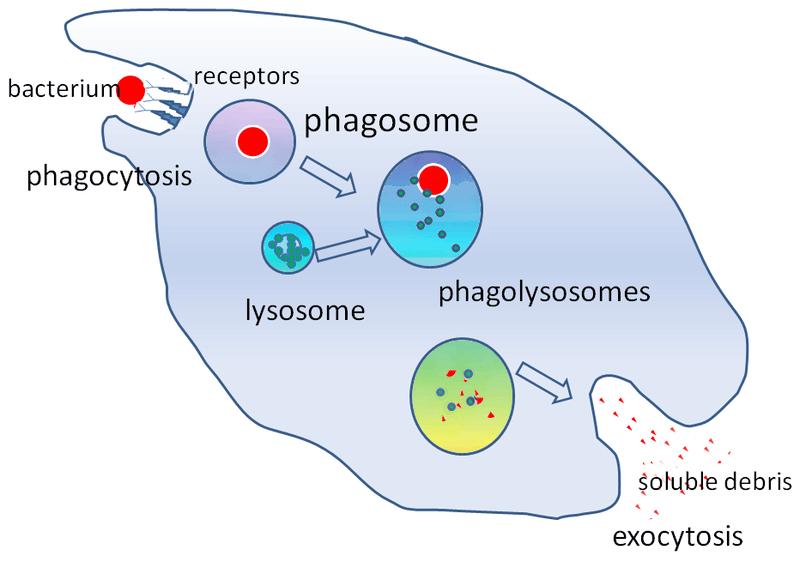
Figure: Steps of phagocytosis
Recognition and attachment:
The efficiency of phagocytosis is greatly enhanced when microbes are opsonized by specific proteins (opsonin).
Major opsonins are
Engulfment:
During engulfment, the extension of the cytoplasm (pseudopods) flows around the particle to be engulfed, resulting in a complete closure of the particle within a phagosome created by the plasma membrane of the cell. The phagocytic vacuole then fuses with the lysosome (phagolysosome), resulting release of the granule content into the phagolysosome.
Killing and degradation:
The killing of microbes is accomplished by
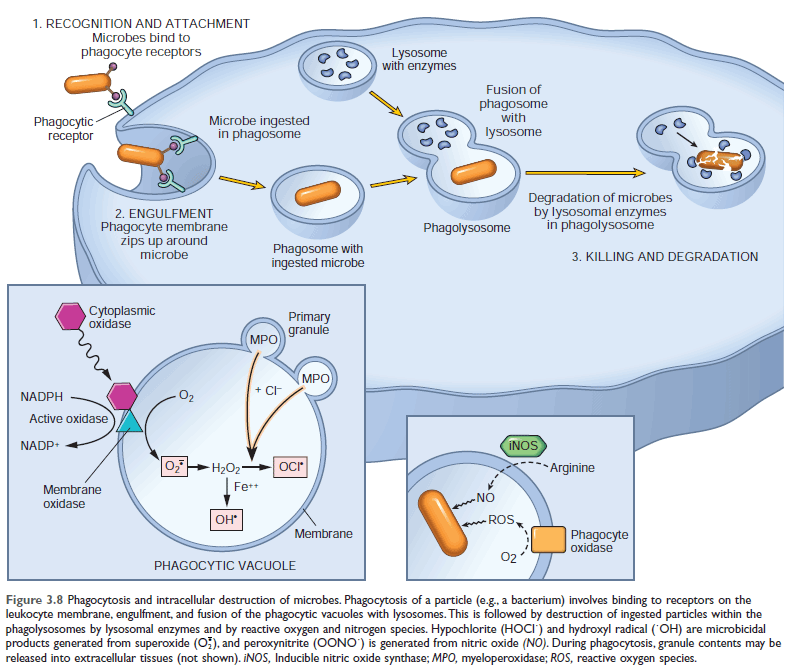
Showing: 1. Phagocytosis process & 2. Production of microbicidal reactive oxygen intermediates within the phagocytic vacuole (Reaction within phagocytic vacuole)
Reactive Oxygen Species:
ROS are produced by the rapid assembly and activation of a multicomponent oxidase, NADPH oxidase (also called phagocyte oxidase), which oxidizes reduced nicotinamide-adenine dinucleotide phosphate (NADPH) and, in the process, reduces oxygen to superoxide anion (O2-).
In neutrophils, this oxidative reaction is triggered by activating signals accompanying phagocytosis and is called the respiratory burst.
(ROS are produced within the phagolysosome, where they can act on ingested particles without damaging the host cell.)
Superoxide (O2-) is then converted into H2O2, mostly by spontaneous dismutation.
H2O2 is not able to efficiently kill microbes by itself. However, the azurophilic granules of neutrophils contain the enzyme myeloperoxidase (MPO), which, in the presence of a halide such as Cl-, converts H2O2 to hypochlorite (HOCl?).
The H2O2-MPO-halide system is the most potent bactericidal system of neutrophils.
H2O2 is also converted to hydroxyl radical (OH), another powerful destructive agent.
|
Is there any problem, if a person is deficient of phagocyte oxidase?
The deficiency of Phagocyte oxidase components (i.e., NADPH oxidase) causes Chronic Granulomatous Disease (CGD) which is an Inherited immunodeficiency disease. |
Nitric Oxide:
NO, a soluble gas produced from arginine by the action of nitric oxide synthase (NOS), also participates in the microbial killing.
In macrophages, NO reacts with superoxide (O2-) to generate the highly reactive free radical peroxynitrite
(ONOO−). These nitrogen-derived free radicals, similar to ROS, attack, and damage the lipids, proteins, and nucleic acids of microbes.
Nitric oxide synthase:
3 types of NOS:
Other functions of Nitric oxide:
Lysosomal Enzymes and Other Lysosomal Proteins
The smaller specific (or secondary) granules contain lysozyme, collagenase, gelatinase, lactoferrin, plasminogen activator, histaminase, and alkaline phosphatase.
The larger azurophil (or primary) granules contain MPO, bactericidal proteins (lysozyme, defensins), acid hydrolases, and a variety of neutral proteases (elastase, cathepsin G, nonspecific collagenases, proteinase
Neutralization of lysosomal enzymes
Destructive effects of lysosomal enzymes (proteases) controlled by antiproteases in serum and tissue fluid.
Example of antiproteases:
Nice to know:
Alpha-1 antitrypsin deficiency (AATD) is an increased risk of having Chronic Obstructive Pulmonary Disease (COPD); which includes Chronic bronchitis & Emphysema
Degradation and clean-up:
After killing, dead microorganisms are degraded by lysosomal acid hydrolases within the phagolysosome.
Neutrophil Extracellular Traps:
Neutrophil extracellular traps (NETs) are extracellular fibrillar networks that concentrate antimicrobial substances at sites of infection and trap microbes in fibril, helping to prevent their spread.
Just To Know:
Culminating Chromatin decondensation – Rupture of the nuclear envelope – Release of chromatin from neutrophil – Forming Extracellular Traps
In this process, the nuclei of the nuclear envelope are lost, leading to the death of cells.
The fate of neutrophils after phagocytosis:
It undergoes apoptotic cell death and is ingested by macrophages.
The peculiarity of phagocytosis:
The contents of lysosomal granules are secreted by leukocytes into the extracellular milieu by diverse mechanisms.
Importance: Can cause further inflammation and tissue injury.
1. Regurgitation during feeding
When phagocytic vacuole remains transiently open to the outside before complete closure of the phagolysosome and releases of lysosomal enzymes to the extracellular fluid.
2. Frustrated phagocytosis:
When the particle is too large to be engulfed or a particle is attached to a surface and cannot be engulfed and released lysosomal enzymes to the extracellular fluid.
Leukocyte-Mediated Tissue Injury:
Leukocytes are important causes of injury to normal cells and tissues under several circumstances.
The function of activated leukocytes
TERMINATION OF THE ACUTE INFLAMMATORY RESPONSE
1. Serous inflammation:
2. Fibrinous inflammation:
3. Purulent (Suppurative) inflammation & Abscess:
4. Ulcer: An ulcer is a local defect or excavation, of the surface of an organ or tissue that is produced by sloughing (shedding) of inflammatory necrotic tissue.
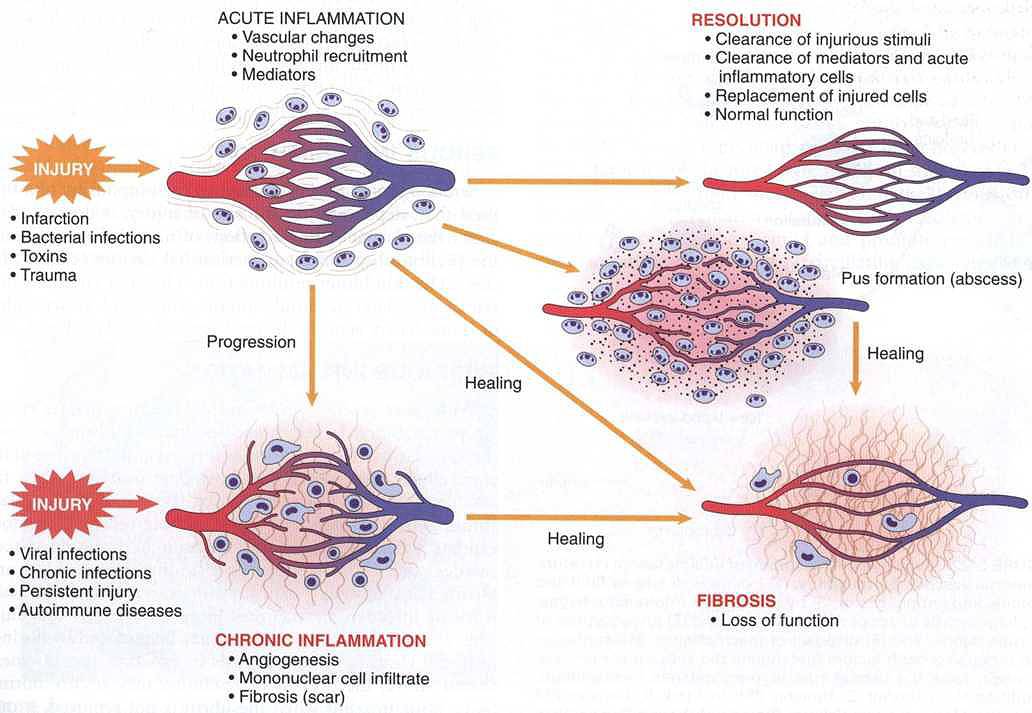
FIGURE 2.21 Outcomes of acute inflammation: resolution, healing by fibrosis, or chronic inflammation
| Site | Inflammation | Site | Inflammation |
| Brain | Encephalitis | Joint | Arthritis |
| Meninges | Meningitis | Subcutaneous tissue | Cellulitis |
| Nerve | Neuritis | Blood vessel | Vasculitis |
| Conjunctiva | Conjunctivitis | Artery | Arteritis |
| Cornea | Keratitis | Vein | Phlebitis |
| Uveal tract | Uveitis | Lymph node | Lymphadenitis |
| Nose | Rhinitis | Lymphatic vessels | Lymphangitis |
| Oral cavity | Stomatitis | Appendix | Appendicitis |
| Salivary gland | Sialadenitis | Cecum | Typhlitis |
| Tonsil | Tonsillitis | Rectum | Proctitis |
| Larynx | Laryngitis | Breast | Mastitis |
| Pharynx | Pharyngitis | Testis | Orchitis |
| Lung | Pneumonia | Ovary | Oophoritis |
| Pleura | Pleurisy | Fallopian tube | Salpingitis |
| Liver | Hepatitis | Prostate | Prostatitis |
| Gall bladder | Cholecystitis | Uterus | Endometritis |
| Muscle | Myositis | Urinary Bladder | Cystitis |
Comments (0)