Postmortem Changes
4 years ago 7596
Forensic taphonomy
Forensic taphonomy is the interdisciplinary study and interpretation of postmortem processes of human remains in the dispositional context, i.e., the history of changes of a body following death.
Knowledge of the signs of death help to differentiate death from suspended animation.
| Types | Changes |
| Immediate changes (somatic) |
Stoppage of nervous system Stoppage of circulatory system Stoppage of respiratory system |
| Early changes (Cellular death) |
Pallor of skin Loss of elasticity of the skin Changes in eye Primary flaccidity of muscle Cooling of body Post mortem staining/lividity Rigor mortis |
| Late changes (decomposition and decay) |
Putrefaction Mummification Saponification (Adipocere formation) |
Medicolegal Important of Late changes after death
Changes in the Skin:
1. The skin becomes pale and ashy-white
2. Loss of elasticity
3. The lips appear dark-red to black, dry, and hard due to drying
4. Contact flattening
Changes in Muscle:
1. Primary flaccidity/relaxation
2. Rigor mortis
3. Secondary flaccidity/relaxation
Changes in the Eyes:
| 1. Loss of corneal reflex |
|
2. Opacity of cornea The opacity is due to drying and is delayed for about two hours if the lids are closed after death. If the eyelids are open for a few hours after death, a film of cell debris and mucus forms two yellow triangles on the sclera at each side of the iris, which become brown and then black called "tache noir" within 3 to 4 hours. ‘Tache noir’ Formation: Due to drying of the eyeball, a film of cell debris and mucus forms a yellow triangular area on the sclera on either side of the iris, which later becomes brown, then black called Tache noir. |
|
4. Pupil: Fixed & dilated, because of the relaxation of muscles of the iris. Pupillary reflex: Absent The pupils react to atropine and eserine for about an hour after death. but they do not react to strong light. |
|
5. Flaccidity of eyeball: Loss of ocular tension (as stoppage of aqueous humor production) |
|
6. Eyelids: Usually, close due to loss of muscle tone |
|
7. Changes in Retina: Segmentation and fragmentation of blood column in retinal vessels Fragmentation or segmentation (tuking or shunting) of the blood columns (Kevorkian sign) in the retinal vessels appear within minutes after death and persists for about an hour. This occurs all over the body due to loss of blood pressure but it can be seen only in the retina by an ophthalmoscope. |
|
9. Chemical change: A steady rise in the potassium values occurs in the vitreous humor after death up to 100 hours. |
Post mortem caloricity
It is a condition in which, instead of cooling of the body, the body temperature remains raised for the first 2 hours or so after death.
Condition/Examples:
1. Post-mortem glycogenolysis
2. Infection's disease: septicemia or bacteremia, excessive bacterial activity, as in septicemia condition, cholera and other fevers
3. Heatstroke
4. High atmospheric temperature
5. Increase in heat production in the muscles due to convulsion as in case of Tetanus and strychnine poisoning
COOLING OF THE BODY (ALGOR MORTIS)
Heat is generated by residual metabolic process (glycogenolysis) of dying tissues and by the metabolic activity of intestinal bacteria, due to which body temperature does not fall for some time.
Internal organs cool primarily by conduction. Conductive heat exchange occurs due to the temperature difference between the body and surroundings. e.g. clothing, covering, air, water, etc. The body heat is mostly lost by conduction and convection.
At non-contact areas heat exchange occurs by convectional mechanism, which exceeds that of the contact surface.
For about half to one hour after death, the rectal temperature falls little or not at all. (postmortem temperature plateau). This is followed by a linear rate of cooling (between 0.4 to 0.6°C per hour) for the next 12 to 16 hours.
The temperature can also be recorded by making a small opening into the peritoneal cavity and inserting the thermometer in contact with the inferior surface of the Iiver.
A rough idea of approximate time in hours of death can be obtained by using the formula:
(Normal body temperature — rectal temperature)/Rate of temperature fall per hour
Variations in rectal temperature:
The rectal temperature is between 36.5 to 37.5°C. Rectal temperature is about 0.6°C higher than oral.
In cases of fat or air embolism, certain infections, septicemia, heatstroke and in pontine hemorrhage, thyrotoxicosis, psychotic (emotional) stress, administration of neuroleptic medication, CO poisoning, intoxication with heroin and cocaine, drug reactions, etc. a sharp rise in temperature occurs.
Factors affecting rate of cooling:
Atmospheric temperature: Greater the difference in temperature between the body and atmosphere, the more rapid in the rate of cooling.
In tropical climates, the heat loss is roughly 0.4°C to 0.6°C and in temperate countries 1°C per hour.
Media of disposal of the dead body: rate of cooling is high in water media, than air and than the grave. The ratio media is water: air: grave: 4:2:1
Body built: The rate of heat loss is proportional to the weight of the body to its surface area. Thus, children and old people cool more rapidly than adults. A thinly built dead body loses heat rapidly and vice versa.
Sex: female bodies retain body heat for a comparatively longer period (due to high subcutaneous fat)
Age: more heat loss in infants.
Clothing or coverings of the body: retain heat for longer period
Air movement: increase air movement- increase rate of cooling
Dry weather: promotes heat loss
Position and posture of the body: in a body with outstretched limbs, the loss of body heat is more.
Post mortem caloricity: it reduces the rate of cooling.
Time of death= (Normal body temperature-Rectal temperature) ÷ Rate of temperature fall per hour
Temperature measurement area in death body
1. Rectum (4 inches above)
2. Sub-hepatic area
3. External meatus & nostril
Medico-legal importance of cooling
Confirmatory sign of death
Time since death can be roughly estimated
Sometimes it indicates the cause of death
It indicates the place of exposure
Different types of stiffening/causes of stiffening:
Rigor Mortis/Cadaveric rigidity/Death stiffening
Cadaveric spasm/Instantaneous rigor
Heat stiffening (due to protein denaturation & coagulation)
Cold stiffening (freezing of the body fluids and solidification of subcutaneous fat simulating rigor.)
Gas stiffening
MUSCULAR CHANGES
After death, the muscles of the body pass through three stages:
(1) Primary relaxation or flaccidity.
(2) Rigor mortis or cadaveric rigidity.
(3) Secondary flaccidity.
Primary Flaccidity:
During this stage, death is only somatic (no cellular death) and it lasts for one to two hours. All the muscles of the body begin to relax soon after death. The lower jaw falls, eyelids loose tension, and joints are flexible.
Body flattens over areas which are in contact with the surface on which it rests (contact flattening).
Muscles are relaxed as long as the ATP content remains sufficiently high to permit the splitting of the actin-myosin cross-bridges.
Muscular irritability and response to mechanical or electrical stimuli persist.
Pupils react to atropine or physostigmine, but not to light.
Rigor Mortis (Cadaveric rigidity/death stiffening)
Appears 1-2 hours after death
It is a state of stiffening of muscles, sometimes with slight shortening of the fibers. Individual cell death takes place in this stage.
The Order of Appearance of Rigor:
All muscles of the body, both voluntary and involuntary are affected.
It does not start in all muscles simultaneously (Nysten's rule).
It first appears in involuntary muscles; the myocardium becomes rigid in an hour.
It begins in the eyelids, neck, and lower jaw and passes upwards to the muscles of the face, and downwards to the muscles of the chest, upper limbs, abdomen, and lower limbs, and lastly to the fingers and toes. In individual limbs, it usually progresses from above downwards.
| Eyelid - Neck |
| Lower jaw |
| Muscles of face |
| Muscles of the chest, upper limbs, abdomen, and lower limbs |
| Lastly to the fingers and toes |
Development:
The development of rigor is concerned with muscles only. It is independent of the integrity of the nervous system, though it is said to develop more slowly in paralyzed limbs.
Diagnosis/Testing of Rigor Mortis
Rigor is tested by trying to lift the eyeLids, depressing the jaw, and gently bending the neck and various joints of the body. Note the degree (absent, minimal, moderate, advanced, or complete) and distribution.
|
1st internally appearance of rigor mortis Myocardium |
|
1st externally appearance of rigor mortis Upper eyelid |
|
The disappearance of Rigor mortis Onset after the putrefaction |
Order of disappearance of Rigor Mortis
Which appears first, that disappear first. Same as the order sequence of appearance of rigor mortis
Eyelids, neck, and lower jaw
muscles of the face—muscles of the chest, upper limbs —abdomen and lower limbs —lastly in the fingers and toes.
Time of Onset:
In India, it begins one to two hours after death and takes a further one to two hours to develop.
Rule of 12:
0-12 hrs — Within this interval, rigor mortis develops, and peaks.
12-24 hrs — Within this interval, rigor mortis remain.
24-36 hrs — Within this interval, rigor mortis disappear progressively.
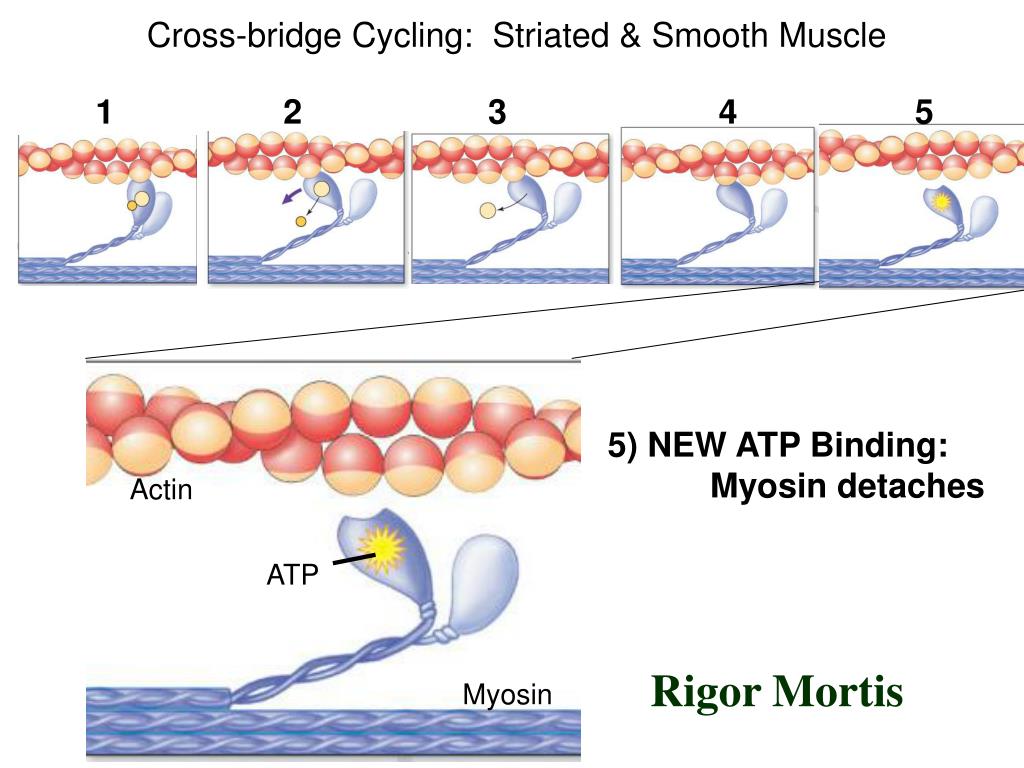
Mechanism
Normally, for the relaxation of a muscle after contraction, ATP is needed.
After death— no further synthesis of ATP which is necessary for relaxation— no separation of actin-myosin complex— causes hardening
During life, the separation of the actin and myosin filaments, and the energy needed for contraction are dependent on adenosinetriphosphate (ATP).
Three metabolic systems are responsible for maintaining a continuous supply of ATP in the muscle:
(1) Phosphagen system
(2) Glycogen-lactic acid system
(3) Aerobic system
The dephosphorylation of ATP by the action of ATPase produces ADP and phosphate, and a large amount of energy, which is used for muscle contraction.
The free phosphate then engages in a phosphorylation reaction that converts glycogen to lactic acid. The lost ATP is replaced during life by resynthesis, which is dependent upon the supply of glycogen.
The lactic acid enters the bloodstream and is reconverted to glycogen in the liver.
At the time of somatic death, enough ATP is present in the muscle to maintain relaxation. After death, the ATP is progressively and irreversibly destroyed leading to increased accumulation of lactates and phosphates in the muscles. There is no resynthesis of ATP.
Postmortem loss of integrity of the muscle cell sarcoplasmic reticulum allows calcium ions to flood the contractile units of the muscle fibers (sarcomeres) initiating the binding of actin and myosin molecules and mimicking the normal contraction process.
Normal relaxation in life is achieved by energy-dependent (ATP-driven) pumping of calcium back across the membrane of the sarcoplasmic reticulum, but this fails after death because of membrane disruption and lack of ATP, due to which increased calcium level in the sarcomeres causes muscle contraction.
When the ATP is reduced to a critical level (85% of the normal), the overlapping portions of myosin and actin filament causes hardness and rigidity of muscle rigor.
The rigidity of the muscle is at its maximum when the level of ATP is reduced to 15%.
The actin-myosin complex is trapped in a state of contraction until it is physically disrupted by the onset of putrefaction.
Medico-legal importance of Rigor mortis
Sign of death
Helps in estimating the time of death
The position of the dead body at the time can be known from contact flattening.
Rigor mortis indicates the molecular death of the muscles involved.
Factors affecting/stimulating rigor mortis:
Age: does not develop in a fetus <7 months intra-uterine age. In healthy adults, it develops slowly but is well-marked and lasts longer, while in children and old people it is feeble and rapid.
Body built/physique of the subject: rigor mortis comes early and passes off early in thinly built subjects with weak musculature.
Atmospheric temperature: at high atmospheric temperature, rigor mortis comes early and passes off early. The onset is rapid due to heat, because of the increased breakdown of ATP, but the duration is short.
In death due to exhaustive disease, or when convulsive proceeds death, rigor mortis appears and passes off early.
In death due to wasting disease, rigor mortis comes early and passes off early.
It may disappear very rapidly in case of widespread bacterial infection, especially in gas gangrene, where putrefaction begins early. Rigor mortis is frequently absent in persons dying from septicemia.
Cadaveric spasm (instantaneous rigor/cataleptic rigidity)
It is a condition in which, the muscles that were contracted during life becomes stiff and rigid immediately after death without passing into the stage of primary relaxation.
The mechanism of cadaveric spasm is obscure but possibly may be neurogenic. Adrenocortical exhaustion which impairs resynthesis of ATP may be a possible cause.
As such, the change preserves the exact attitude of the person at the time of death for several hours afterwards.
No other condition simulates cadaveric spasm and it cannot be produced by any method after death. It passes without interruption into normal rigor mortis and disappears when rigor disappears.
Causes/Predisposing Factor
Sudden death
Intense physical and/or emotional activity such as excitement, fear, severe pain, exhaustion,
Cerebral hemorrhage, Injury to nervous system
Firearm wound of the head, Drowning
Convulsant poison e.g., strychnine
Medico-legal importance of cadaveric spasm
Occasionally, in case of suicide the weapon e.g., pistol of knife is seen in the victim's hand which is a strong evidence of suicide.
If the deceased dies due to assault, some part of clothing e.g., button of his assailant or some hair may be firmly grasped in the hands.
In case of drowning: grass, weeds or leaves may be found firmly grasped in the hands, which indicates that the victim was alive on entering the water.
Difference between rigor mortis and cadaveric spasm:
| Traits | Rigor mortis | Cadaveric spasm |
| Onset | 1-2 hours after death | Just after death (Instantaneous) |
| Muscle involves | All muscles (both voluntary & involuntary) | Usually a single group of voluntary muscle |
| Production | Freezing & exposure to temp.above 65C will produce rigor | Cannot be produced by any method after death |
| Death of muscle | Molecular death | No molecular death |
| Electric stimuli | Muscles do not respond | Muscle respond |
| Predisposing factor | No | Sudden death, excitement, fear, exhaustion, nervous tension, |
| Body temperature | cold | Warm |
| Muscle reaction | Acidic | Alkaline |
| Mechanism | ATP | unknown |
| Medico-legal importance | Indicates time of death | Indicates manner of death i.e suicide, homicide or accident |
CONDITIONS SIMULATING RIGOR MORTIS
1. Heat Stiffening:
When a body is exposed to temperatures above 65°C. a rigidity is produced, which is much more marked than that found in rigor mortis. It is seen in deaths from burning, high voltage electric shock and from falling into hot liquid. Heat causes stiffening of the muscles, because the tissue proteins are denatured and coagulated as in cooking. Coagulation of protein is seen in burns on microscopic examination
The stiffening remains until the muscles and ligaments soften from decomposition and the normal rigor mortis does not occur.
2. Cold Stiffening:
When a body is exposed to freezing temperatures before acid metabolites appear in the muscles, the tissues become frozen and stiff, due to freezing of the body fluids and solidification of subcutaneous fat simulating rigor.
If the body is placed in the warm atmosphere, the stiffness disappears and after a time, the normal rigor mortis occurs rapidly and passes off quickly.
3. CADAVERIC SPASM or Instantaneous Rigor:
Cadaveric spasm (cataleptic rigidity) is a rare condition. In this, the muscles that were contracted during life become stiff and rigid immediately after death without passing into the stage of primary relaxation. As such, the change preserves the exact attitude of the person at the time of death for several hours afterwards.
Secondary Relaxation:
Flaccidity following rigor mortis is caused by the action of the alkaline liquids produced by putrefaction. Another view is that rigidity disappears due to solution of myosin by excess of acid produced during rigor mortis. A third view is that enzymes are developed in dead muscle which dissolve myosin by a process of auto-digestion.
Hypostasis (Postmortem staining) Time: well-developed within 4 hrs & reaches maximum in 6-12 hrs
This is the bluish-purple or purplish-red (due to deoxyhemoglobin) discoloration, which appears under the skin in the most superficial layers of the dermis of the dependent parts of the body after death, due to capillo-venous distention.
It is also called postmortem staining, subcutaneous hypostasis, livor mortis, cadaveric lividity, suggestions, vibices, and darkening of death.
Mechanism:
It is caused by the stoppage of circulation, the stagnation of blood in blood vessels, and its tendency to sink by force of gravity.
The intensity of the color depends upon the amount o f reduced hemoglobin in the blood. In cases of large amount of reduced hemoglobin before death, the blood has deep purplish-red color.
Development:
Postmortem lividity begins shortly after death, but it may not be visible for about half to one hour after death in normal individuals.
It is usually well developed within four hours and reaches a maximum between 6 to 12 hours (primary lividity) and persists until putrefaction sets in.
The physical factors for fixation of post mortem staining are:
(l) Blood cannot pass out of the capillaries after formation of p.m. hypostasis.
(2) Rigor mortis obliterates the big vessels, and as such the blood cannot pass through these vessels to settle in venules and capillaries in a new area.
(3) After full development of rigor mortis, venules and capillaries are compressed and almost empty and cannot be easily distended by the resettling blood. Hypostasis becomes fixed when blood leaks into the surrounding soft tissues due to hemolysis and breakdown of blood vessels.
Hypostasis may be sparse or even absent in deaths where considerable blood loss of at least 65% of the circulating blood volume in adults and 45% in infants, occurs before death due to trauma. In severe anaemia lividity will be absent.
Internal Hypostasis:
Hypostasis also occurs in the dependent parts of internal organs. When a body is in supine position, hypostasis is seen in the posterior portions of the cerebrum and cerebellum, the dorsal portions of the lungs, posterior wall of the stomach, dorsal portions of the liver, kidneys, spleen, larynx, heart, and the lowermost coils of intestine in the pelvic cavity.
Medico-legal importance of hypostasis
It is a sign of death
Its extent helps in estimation of time since death (unreliable)
It indicates the posture of the body at the time of death.
It may indicate moving of the body to another position sometime after death.
Sometimes, the color may indicate the cause of death.
Different color markings in a dead body:
| Ante-mortem origin | Post- mortem origin | Artificial |
|
1. Trauma: bruise and traumatic asphyxia 2. Asphyxia: cyanosis 3. Inflammation: congestion in organs or skin 4. Emboli: fat embolism 5. Physical: exposure to severe cold and heat |
1. Hypostasis 2. Putrefaction 3. Poisoning: CO, HCN, Nitrates, chlorate,etc |
1. Paint 2. Grease 3. Dust 4. Mud 5. Coal 6. Blood 7. semen |
Putrefaction
It is a process of liquefaction of elements or compound due to action of fermentation process or due to autolysis.
Decomposition= putrefaction+autolysis
The disintegration of body tissues after death is known as decomposition. The terms decomposition and putrefaction are used as synonyms. Putrefaction usually follows the disappearance of rigor mortis.
Mechanism of putrefaction:
| Action of micro-organism |
After death— O2 tension of the tissue reduces--anaerobic micro-organisms(within the body and environment) grow— they break tissue protein, fat and carbohydrates and production of foul—smelling gases- putrefaction proceeds. (micro-organisms: clostridium welchii, E. coli, Staphylococcus, nonhemolytic streptococcus, diphtheroid and proteus are the important ones) |
| Autolysis | After death cell membrane ruptures— release of cytoplasmic enzymes — breakdown of tissue CHO, protein, fat and other substances- tissue degradation- putrefaction proceeds. |
Mechanism:
Organisms enter the tissues shortly after death, mainly from the alimentary canal, and less often through the respiratory tract or through an external skin wound.
The fall in the oxygen concentration in the tissues and rise in hydrogen ion concentration after death favor bacterial growth and spread throughout the body. Because the protective agencies of the body are absent, the bacteria spread through the blood vessels using the proteins and carbohydrates of the blood as culture media.
Destruction is caused mainly by the action of bacterial enzymes, mostly anaerobic organisms derived from the intestines. The chief destructive bacterial agent is Cl. welchii, which causes marked hemolysis, liquefaction of postmortem clots and of fresh thrombi and emboli, disintegration of tissue and gas formation in blood vessels and tissue spaces.
Lecithinase(enzyme) produced by Cl. welchii is most important. This hydrolyses the lecithin which is present in all cell membranes including blood cells·, and is responsible for the postmortem hemolysis of blood.
The other organisms include Streptococci, Staphylococci, bacteroids, anaerobic lacbobacilli , diphtheroids, Bacillus proteus, B. coli., B. aerogenes capsulatus, etc.
Stage's putrefaction:
| No. | Stages | Time |
| 1. | Color change appears in | Summer: 12-18 hours; winter:1-2days |
| 2. | Development of foul smelling | Summer: 12-18 hours; winter: 1-2 days |
| 3. | Appearance of maggots | Larvae: 8-24 hours; pupae: 4-5days |
| 4. |
Colliquative putrefaction (Liquefaction of Tissue) |
5-10 days |
Maggots are produced in one to 2 days which have proteolytic enzymes that dissolve the tissue.
The marbling of Skin:
The superficial veins especially over the roots of the limb, thighs, sides of the abdomen, shoulders, chest and neck are stained greenish-brown or purplish-red depending on the total amount of sulphhaemoglobin formation within the affected vessels (linear branching pattern) due to the hemolysis of red cells, which stains the wall of the vessel and infiltrates into the tissue, giving a marbled appearance (red, then greenish pattern in skin resembling the branches of a tree)
Development of Foul-smelling Gases:
The chemical processes in this stage are those of reduction, the complicated proteins and carbohydrates being split into simpler compounds of amino acids, ammonia, CO, CO2, hydrogensulphide,phosphorated hydrogen, methane and mercaptans.
Names of Putrefactive Gases:
1. Hydrogen Sulphide (Important)
2. Ammonia
3. Methane
4. CO, CO2
6. Phosphorated hydrogen
As a general rule, the organs show putrefactive changes in the following order.
(l) Larynx and trachea (12-24hrs)
(2) Stomach, intestines, pancreas and spleen
(3) Liver, lungs.
(4) Brain.
(5) Heart.
(6) Kidneys, bladder.
(7) Prostate, uterus.
(8) Skin, muscle, tendon.
(9) Bones.
1st External sign of appearance of decomposition
Right Iliac fossa
(Skin over the caecum)
Why?
1. Contents of the bowel are more fluid and full of bacteria.
2. Caecum lies superficially near the skin
Greenish discoloration of the skin over the region of the caecum
Due to conversion of hemoglobin of blood into sulphmethaemoglobin by the hydrogen sulphide formed in the large intestine and escaping into the surrounding tissues.
1st Internal appearance of decomposition
Aorta intima
Undersurface of liver
1st organ to decomposed
Larynx & trachea
Then stomach, intestines
Last organ to decomposed
Uterus (in female)
Prostate (in male)
How to differentiate sex in death body in decomposed body.
Finding of uterus or prostate, because these uterus & prostate are the last organ to decomposed
In advanced decomposed, if these organs cannot be found, then other examination.
Medicolegal importance of putrefaction
Time since death can be estimated from the stages of decomposition.
Advanced decomposition may obliterate the identity of the dead.
Advanced decomposition may also obliterate the cause of death.
How to diagnose decomposition?
Feature/cardinal signs/characteristics of putrefaction:
Changes in the color of tissues
The evolution of the gases in the tissues.
The liquefaction of the tissues
Last change in decomposition is liquefaction.
Factor influence decomposition in water
Water temperature
Stagnancy of water— in stagnant water, decomposition is rapid than flowing water.
Quality of water— Decomposition is slow in fresh water
Aquatic animals — will favor the decomposition
Factors influencing floatation of dead body on water
Early Decomposition
Salty water more sp.gravity
Stagnant water
Clothing, Sex(Female)
Effects (Pressure) of Putrefaction
Difficulty in identification
Distention of body cavities & hallow organs
Discharge if forth fluid from mouth & nostrils.
Formation of post mortem blister due to accumulation of gas under epidermis
Gas stiffening
Explusion of food particles and feces through anus
If deceased was pregnant, post mortem delivery may occur
Difference between Ante-Mortem and Post mortem blister:
| Traits | Ante-mortem | Post-mortem |
| Fluid | More | Less |
| Transparency of fluid | Clear | Reddish |
| Presence of albumin | Rich | Poor |
| Zone of inflammation | Red Ring present | Absent |
| Base of the floor | Velvety appearance | White and glistening |
Mummification
It is a late post-mortem change in which there is rapid drying of the dead body due to some environmental factors, when the soft tissues become dark, hard and stay preserved. The dry, hard skin gets almost adhere with the underlying bones is known as mummification.
Rapid drying & shriveling of the dead body due to evaporation of water but the natural appearances of the body and general facial features are preserved.
Time: 3 months to 1 years
Requirement for mummification
Dry weather
Hot atmosphere
Absence of moisture
Free of air movements
Influencing factors of Mummification
Hot atmosphere
Dry atmosphere
Free air movement
Contact of body with absorbing media
Medico- legal importance Mummification
It gives a rough idea about the time since death.
Identification: in this condition the body is not grossly destroyed and many identification features like old scars, deformities, tattoo marks etc. can be detected after a long time.
Cause of death: as the body is not grossly destroyed, injuries can be detected after a long time.
The place of disposal of the dead body after death can be guessed (dry hot place with absorbing type of soil, etc.)
Saponification (adipocere formation)
Formation of soft, whitish, crumbly, waxy and greasy materials occurring in fat/fat containing tissue of a dead body.
Adipocere (cire=wax) is a modification of putrefaction. In this, the fatty tissues of the body change into a substance known as adipocere. It is seen most commonly in bodies immersed in water or in damp, warm environment.
Mechanism of Saponification
Due to hydrolysis & hydrogenation of body fats. The process needs water, and at initial phase utilizes the body fluid..
The chemical reaction involves change of fat to higher fatty acid like palmitic acid, stearic acid.
Mechanism:
The change is due to the gradual hydrolysis and hydrogenation of pre-existing fats, such as olein, into higher fatty acids, which combine with calcium and ammonium ions to form insoluble soaps, which being acidic, inhibit putrefactive bacteria.
Ultimately, the whole of the fat is converted into palmitic, oleic, stearic and hydroxystearic acid, together with some glycerol, and a mixture of these substances forms adipocere.
The process starts under the influence of intrinsic lipases, and is continued by the bacterial enzymes of the clostridia group, mainly Cl. perfringens, as the bacteria produce lecithinase, which facilitates hydrolysis and hydrogenation . Water is essential for the bacterial and enzymatic processes involved in adipocere formation.
Factor influencing saponification
Atmospheric temp. Heat favor it
Moisture favor
Air movements inhibit the process
Running water inhibit it
Medico-legal importance of Saponification
1) When the process involves the face, the features are well preserved, which help to establish the identity.
(2) The cause of death can be determined, because injuries are recognized.
(3) The time since death can be estimated.
Maceration
Process of aseptic autolysis of dead fetus occur when the dead child remains in the uterus for about 3,4 days surrounded with liquor amine but the exclusion of air
Difference between putrefaction & maceration
| Putrefaction | Maceration | |
| Mechanism | Action of microorganisms and autolysis | Aseptic autolysis |
| Site of occurrence | Out side of uterus | Inside the uterus |
| Role of air | Enhance the process | No role or inhibit it |
| Smell | Offensive foul smell | Sweetish |
| Color of skin | Green | Red or purple |
| Condition of viscera | Soft & flabby | Soft & edematous |
CONDITIONS PRESERVING THE BODY
1. Embalming is the treatment of the dead body with antiseptics and preservatives to prevent putrefaction and preserve the body. By this process proteins are coagulated, tissues are fixed, organs are bleached and hardened and blood is converted into a brownish mass. Embalming produces a chemical stiffening similar to rigor mortis, and normal rigor does not develop. Embalming rigidity is permanent.
Formalin (Preservative)
Sodium borate (Buffer)
Sodium citrate (Anticoagulant)
Glycerin (Wetting agent)
Sodium chloride (Controls pH)
Eosin (1%, Cosmetic)
Soluble wintergreen (Perfume)
Water (Vehicle)
2) Mummification.
(3) Adipocere formation.
(4) Freezing
Difference between post mortem staining and Bruise
| Post mortem staining | Bruise | |
| Situation | On the dependent part of dead body | Anywhere |
| Tissue level | Under the skin | Subcutaneous level |
| Causes | Due to capillo-venous distention with blood | Due to extravasation of blood from capillaries |
| Effect of pressure | Pressed spot appears pale | No change |
| Cut section | Cut surface show oozing of blood from smaller vessels which can be cleaned by washing | Cut surface shows evidence of hemorrhage in the tissue which cannot be washed out (in dead bodies) |
| Medico-legal imp | Tells about the time of death and position of dead body | Tells about the nature of injury, weapon, used, etc. |
Difference between post mortem staining & congestion
| Post mortem staining | Congestion | |
| Situation | Dependent part of organ | Whole part if organ, affected with pathology |
| Cut surface | Oozing of blood from distended capillaries | Exudation of fluid mixed with blood from cut surface |
| Cause | Passive capillovenous distension | Due to some pathology in organ |
| Nature | Post-mortem | Ante-mortem |
| Swelling | Nil | May present |
Difference between Rigor Mortis &Heat stiffening
| Rigor Mortis | Heat stiffening | |
| Mechanism of formation | Due to depletion of ATP in muscle | Due to heat coagulation of protein |
| Time | 1-2hrs after death |
May be ante-mortem or post-mortem Formed due to contact with heat |
| Role of heat | Atmospheric high temperature enhances the process | Temp above 65 C |
| External appearance | Nothing specific | Sign of exposure to heat will be there like burning, blister formation |
Difference between Primary & Secondary Relaxation
| Primary relaxation | Secondary relaxation | |
| Time | Immediately after death | After rigor mortis passes off & decomposition occurs |
| Death of muscle | Has not occurred | Molecular death has occurred |
| Respond to stimuli | Respond | Does not respond |
| Body temperature | Near normal | Low |
| Other external features | Not particular | Sign of decomposition present |
- Estimation of time since death:
1. Cooling of the body: starts from ½ to 1 hour after death
2. Cadaveric hypostasis: starts from 1 hour after death and well-marked within 5-12 hours.
3. Rigor mortis: instantaneous with death
4. Adipocere formation
5. Mummification
6. Degree of digestion of stomach contents
7. Condition of bladder
8. C.S.F
9. Bone marrow
10. Blood3. Saponification (Adipocere formation)
Comments (0)