Anterior Abdominal Wall
5 years ago 2899
| Above: Xiphoid process left and right costal margin |
| Below: Anterior part of the iliac crest, Fold of the groin, Pubic tubercle, pubic crest, and symphysis pubis |
| On each side: Mid-axillary line separates it from the posterior wall |
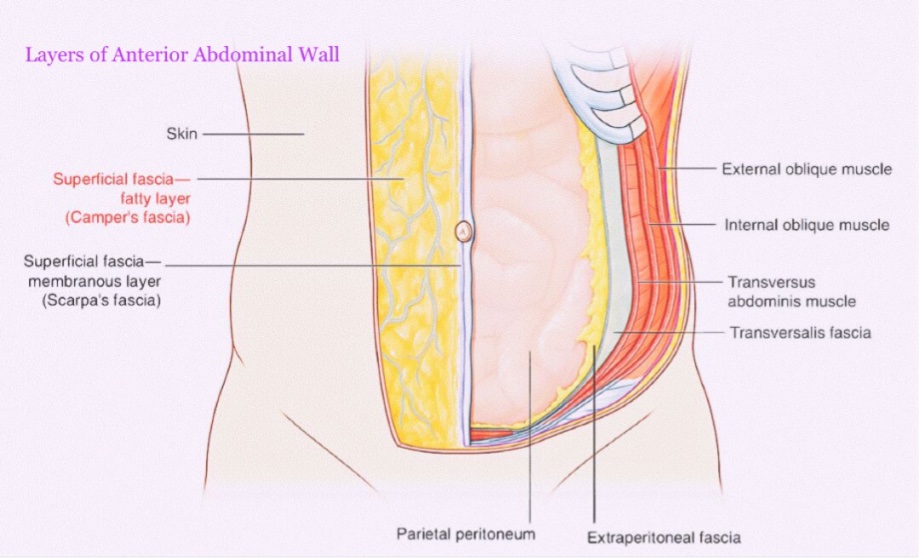
Layers of the anterior abdominal wall
Why deep fascia is absent in the anterior abdominal wall?
To allow the bulging/distension of the abdominal wall as after taking meals, during pregnancy, etc.
It also absents in the penis, scrotum, and perineum.
Nice to know:
| The first layer of the anterior abdominal wall is the skin. It has cleavage lines called the Langer's lines which are important for cosmetic surgery. |
| The umbilicus is formed from cicatricial tissue and represents the umbilical cord remnant. |
| The second layer of the anterior abdominal wall is the superficial fascia. |
| It consists of 2 layers:- 1) Fascia of Camper- contains subcutaneous fat 2) Fascia of Scarpa- made of elastic fibrous tissue |
| Between the 2 layers, there are a number of structures like- superficial epigastric, superficial circumflex iliac and superficial external pudendal vessel, the femoral artery, femoral vein, superficial inguinal lymph nodes. |
Muscles of the anterior abdominal wall :
| Flat muscles : |
| External oblique muscle Internal oblique muscle Transversus abdominis muscle |
| Vertical muscles : |
| Rectus abdominis muscle Pyramidalis muscle |
Structures derived from flat muscles :
1. Inguinal ligament
2. Conjoint tendon
3. Cremaster muscle.
Cutaneous nerves of the anterior abdominal wall :
Anterior Cutaneous branches:
They (seven in number) are derived from the lower five intercostal, subcostal, and iliohypogastric nerve.
Lateral Cutaneous Branches:
The lateral cutaneous branches derived from the lower two intercostal, subcostal, and iliohypogastric nerves.
Arteries of the anterior abdominal wall :
Veins of the anterior abdominal wall :
Lymphatics of the anterior abdominal wall :
Rectus sheath :
Definition:
The rectus sheath is an aponeurotic sheet enclosing the rectus abdominis muscle on each side of the linea alba. It is derived from the aponeuroses of flat muscles of the anterior abdominal wall.
Features:
The rectus sheath presents anterior & posterior wall -
Anterior wall :
| It is complete and covers the entire extent of muscles. |
| It is firmly adherent to the tendinous intersection of the rectus muscle. |
Posterior wall :
| It is incomplete, being deficient above the costal margin and below the arcuate line. |
| It is free from the rectus muscle. |
Steps of dissection :
| A longitudinal incision from the xiphisternal junction up to the symphysis pubis in the midline making a semicircular incision around the umbilicus on the dissected side. |
| A transverse incision from the upper end of the first incision to the laterally for about 3 cm. |
| An oblique incision from the lower end of the first incision along the inguinal ligament up to its midpoint. |
| Then the skin reflected laterally. |
| Then the superficial fascia is reflected laterally. |
Formation :
Above the level of costal margin:
| Anterior wall: By the aponeurosis of external oblique only. |
| Posterior wall: It is deficient and muscle lies directly on the 5th-7th costal cartilages. |
Between coastal margin and arcuate line:
| Anterior wall: By the fusion of aponeurosis of external oblique with the anterior lamina of aponeurosis of internal oblique. |
| Posterior wall: By the fusion of aponeurosis of transversus abdominis with the posterior lamina of aponeurosis of internal oblique. |
Below the level of arcuate line:
| Anterior wall: By the aponeuroses of all the three flat muscles (the aponeurosis of transversus abdominis and internal oblique are fused but the aponeurosis of external oblique remains separate). |
| Posterior wall: It is deficient. |
Contents :
| Two muscles: 1. Rectus abdominis 2. Pyramidalis (if present) |
| Two arteries: 1. Superior epigastric artery 2. Inferior epigastric artery. |
| Two veins: 1. Superior epigastric vein 2. Inferior epigastric vein. |
| Six nerves: Terminal parts of lower six thoracic nerves, including lower five intercostal nerves and subcostal nerve. |
Functions :
1. Checking the bowing of rectus abdominis muscle during its contraction and hence increasing its efficiency.
2. Maintaining the strength of the anterior abdominal wall.
Abdominal region :
The abdominal cavity is divided into nine regions by four imaginary planes (two vertical and two horizontal) on the anterior abdominal wall.
Superior horizontal plane or transpyloric plane:
It is placed midway between the suprasternal notch and the pubic symphysis. The transpyloric plane lies at the level of the lower border of the L1 vertebra and cuts the costal margin at the 9th costal cartilages.
Inferior horizontal plane or intertubercular plane:
It is drawn at the level of tubercles of the iliac crests, which are palpable 5 cm posterior to the anterior superior iliac spine. The intertubercular plane lies at the level of the upper border of the L5 vertebra.
Right and left vertical planes or midclavicular planes:
Each vertical plane passes vertically downward from the midpoint of the clavicle to the mid-inguinal point (a point midway between the anterior superior iliac spine and the pubic symphysis).
Inguinal region.
Definition:
It is the area of junction between the anterior abdominal wall and the anterior aspect of the thigh.
It extends between the anterior superior iliac spine and pubic tubercle.
Why inguinal region is important anatomically?
Some structures enter and exits from the abdominal cavity through the region.
Why Inguinal region is clinically important?
Because hernia affects this region(inguinal hernia and femoral hernia)
Inguinal ligament
It's a fibrous band.
Length: About 12 to 14 cm.
How does inguinal ligament form?
It is formed by the backward folding of the external oblique aponeurosis on itself.
Attachment
Laterally: Anterior superior iliac spine
Medially: Pubic tubercle.
What are the structures attached to the Inguinal ligament?
| Lateral two-third: Internal oblique muscle |
| Lateral one third: Transversus abdominis |
| Middle third: Cremasteric muscle |
| Inferior surface: Fascia lata (Deep fascia of thigh) |
Structures passing below the inguinal ligament.
| Muscles: Iliopsoas Pectineus |
| Vessels: Femoral vessels Inferior epigastric vessels Deep circumflex iliac vessels |
| Nerves: Femoral nerve Genitofemoral nerve |
| Lymphatic vessels |
| Femoral sheath |
Inguinal canal
It is an oblique muscular passage, about 4cm in length, and extends from the deep inguinal ring to the superficial inguinal ring.
Situation:
It is just above and parallels with the medial half of the inguinal ligament.
Direction:
It is directed downwards, forwards, and medially.
Inguinal canal is larger in males than in females.
Which wall of the inguinal canal is weak?
Posterior wall
Peculiarities :
In females the canal is narrow.
In the newborn, the canal is directed almost straight forwards because muscles of the anterior abdominal wall are not properly differentiated.
Boundaries
| Anterior wall: Entirely formed by Skin Superficial fascia External oblique aponeurosis |
| Lateral one-third: Fleshy fibers of the internal oblique. |
| Posterior wall: Entirely formed by fascia transversalis Parietal peritoneum Extra peritoneal |
| Medial half: Conjoint tendon |
| Medial one-forth: Reflected part of the inguinal ligament |
| Roof: Formed by the arched fibers of the internal oblique and transversus abdominis muscles. |
| Floor: Formed by the grooved upper surface of the inguinal ligament. |
Inguinal canal
| Inlet is formed by the deep inguinal ring. |
| Outlet is formed by the superficial inguinal ring. |
Deep inguinal ring:
It is an oval opening in the fascia transversalis.
Situation: 1.25 cm above in the mid inguinal point.
Superficial inguinal ring:
It is an oblique triangular gap in the aponeurosis of the external oblique.
Situation: Just 1cm above and lateral to the pubic crest.
Content
In case of male:
1. Spermatic cord.
2. Ilioinguinal nerve.
In case of female
1. Round ligament.
2. Ilio-inguinal nerve.
Spermatic cord
It is a collection of structures that pass to and fro from the testis through the inguinal canal.
Length: It is about 7.5 cm.
Extensions:
It extends from the deep inguinal ring to the upper part of the posterior border of the testis.
Coverings:
From within outwards
1. Internal Spermatic fascia
2. Cremasteric fascia
3. External spermatic fascia
Contents:
| Arteries Testicular artery Cremasteric artery Artery of the Ductus deferens |
| Veins: Pampiniform plexus of veins. |
| Nerves: Ilio-inguinal nerve Genital branch of the genitofemoral nerve |
Hernia
Protrusion of a viscus from its abnormal position.
Parts of hernia:
1) Hernial sac
2) Content of sac
3) Coverings of the sac
Inguinal hernia
Protrusion of any abdominal contests or viscera from its normal position to the inguinal canal, then it is called an inguinal hernia.
Inguinal hernia is common in males.
Types:
1. Direct inguinal hernia
2. Indirect inguinal hernia.
Indirect inguinal hernia
When the abdominal viscera/content comes into the inguinal canal through the deep inguinal ring is called an indirect inguinal hernia.
Causes: Congenital
Indirect hernia may occur in children and young adults.
Usually unilateral.
Direct hernia
When the abdominal viscera/content comes into the Inguinal canal through the posterior wall of the inguinal canal or Hesselbach's triangle, it's called a direct inguinal hernia.
Causes: Due to weakness of the muscles of the anterior abdominal wall.
Direct hernia occurs in old age.
It is bilateral
Importance of Linea Alba
The supraumbilical median incisions are made on the linea Alba because it is bloodless &safe to muscles and nerves.
Also read: Anatomy Question Collection
Also read: Anatomy Questions & Answers
Also read: Anatomy notes
Comments (0)