Ribs & Intercostal Space (Viva)
6 years ago 4864
RIBS
Q.1 What are ‘True ribs’?
First seven ribs connected through costal cartilages to the sternum are called true ribs.
Q.2 What are ‘false ribs’?
Q.3 What are typical and atypical ribs?
First two and last three ribs are called atypical because they present special features. The 3rd to 9th ribs are called typical because they have common features.
Q.4 What are the features of a typical rib?
Each typical rib has
Q.5 What are the relations of the head of a typical rib?
Q.6 What is a costal groove? Name the structures attached and lying within the costal groove?
Costal groove is a depression present between the inferior border and the ridge on the inner surface.
Attachments:
Origin of internal intercostal muscle from floor of groove.
Contents:
From above downwards:
Q.7 What are the special features of 1st rib?
Q.8 Name the structures related to the neck of the first rib.
Anteriorly from medial to lateral side:
Superiorly:
Q.9 What are the structures related to grooves on the superior surface of the first rib?
Q.10 What is the difference in ossification of 1st and other typical ribs?
The typical ribs have three secondary centers, one for head and two for tubercle. The first rib has two secondary centers, one for head and one for tubercle.
Q.11 What are the special features of 2nd, 10th, 11th, and 12th rib?
Second rib:
Tenth rib:
Eleventh rib:
Twelfth rib:
Q.12 In which rib both superior and inferior costotransverse ligaments are absent?
12th rib
Q.13 What is the characteristic of the costovertebral joint of 1st, 10th, 11th, and 12th ribs?
These ribs articulate only with corresponding vertebrae.
Q.14 What is the commonest site of rib fracture in adults?
The rib is fractured at the angle, which is its weakest point.
Q.15 Why the fracture of ribs are rare in children?
Because in the children the chest wall is highly elastic.
Q.16 What is ‘Stove in chest’?
This is produced in severe crush injuries in which multiple rib fractures are produced along with permanent indentation of the chest wall.
Q.17 What is ‘Flail chest’?
This results from more severe injury to chest. Multiple rib fractures at two or more sites result in an unstable chest wall in which the Flail area is sucked inwards during inspiration and pushed out in expiration.
Q.18 What is cervical rib?
Q.19 What is the clinical importance of a cervical rib?
It may press on the lower trunk of brachial plexus producing paraesthesia along the ulnar border of forearm and wasting of small muscles of the hand. Less commonly, vascular changes are produced due to pressure on the subclavian artery.
Q.20 What is the histological structure of costal cartilage?
It is made up of hyaline cartilage.
Q.21 What type of joints costal cartilage form?
INTERCOSTAL SPACES
Q.1 What are intercostal spaces?
Gaps between ribs and their costal cartilages are called intercostal spaces.
Q.2 What are typical intercostal spaces?
The 3rd to 8th spaces are typical intercostal spaces. The blood and nerve supply of 3rd to 6th intercostal space is limited only to the thoracic while those of lower spaces extend into the abdomen.
Q.3 What are the contents of a typical intercostal space.
Q.4 What is the attachment and extent of external intercostal muscle?
Attachment:
Q.5 What is the attachment and extent of internal intercostal muscle?
Origin:
Floor of the costal groove of the rib above.
Insertion:
Inner lip of the upper border of the rib below.
Fibers are at right angles to those of external intercostal.
Extent:
From the lateral margin of the sternum to the angle of the rib where it continues as the internal intercostal membrane.
Q.6 Name the muscles which comprise the transversus thoracic group of muscles.
Q.7 What is the attachment of muscles comprising the transversus thoracic group of muscles?
They form the innermost layer of the muscles of the thoracic wall.
They arise from the lower part of the posterior surface of the body of the sternum and the xiphoid process and the adjacent costal cartilages (4th to 7th). They pass upwards and laterally and are inserted by slips to the costal cartilages of the 2nd to 6th ribsThe direction of fibers of these three parts is the same as internal intercostal muscle.
Q.8 What is the position of neurovascular plane of the thorax?
Between internal intercostal muscle and intercostalis intimi and posteriorly between pleura and internal intercostal membrane.
The vein is highest, artery is in the middle and the nerve is lowest.
Q.9 What will happen if intercostal muscles are paralyzed?
There will a retraction of intercostal spaces during inspiration and bulging during expiration.
Q.9.1 How intercostal nerves are formed and how they are distributed?
These are the ventral primary rami of T1- T11 nerves. The ventral primary rami of T12 forms the subcostal nerve.
T1 and T2 supply the upper limb.
T3 to T6 supply thoracic wall (Typical intercostal nerves).
T7 to T11 supply abdominal wall
Q.10 What are the branches of a typical intercostal nerve?
– White ramus communicans
Connected to
– Grey ramus communicans sympathetic ganglion.
– Muscular branches:
Supplies intercostal muscles, serratus posterior superior.
– Collateral branch:
Supplies intercostal muscles, parietal pleura, and periosteum of rib.
– Lateral cutaneous branch:
Emerges at the midaxillary line. Divides into anterior and posterior branches.
– Anterior cutaneous branch:
Emerges at the lateral border of the sternum.
Q.11 What is the characteristic feature of the second thoracic nerve?
Its lateral cutaneous branch forms the intercostobrachial nerve which enters the upper limb and supplies the skin on the medial side of the upper arm.
Q.12 Where the pain due to irritation of intercostal nerves is referred to?
To the front of the chest or abdomen, i.e., at the peripheral termination of nerve.
Q.13 What is the course of pus from the vertebral column around the thorax?
The pus may track along the course of the neurovascular bundle and may point at the exit of cutaneous branches of intercostal nerve, i.e., lateral to erector spinae, in mid axillary line and just lateral to the sternum.
Q.14.1 Name the arteries of intercostal space.
Q.14 Name the branches of posterior intercostal arteries?
Q.15 What is the origin of intercostal arteries?
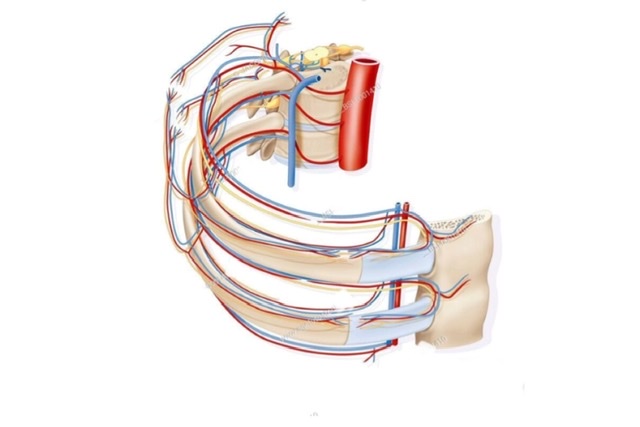
Q.16 How the intercostal veins terminate?
| On the left side: |
| 1st: Into the left brachiocephalic vein. 2nd and 3rd: Form left superior intercostal vein which drains into the left brachiocephalic vein. 4th to 8th: Into accessory hemiazygos vein. 9th to 11th and subcostal veins: Into hemiazygos vein. |
| On the right side: |
| 1st: Into the right brachiocephalic vein. 2nd and 3rd: Form right superior intercostal vein which drains into the azygos vein. 4th to 11th and subcostal vein: Into azygos vein. |
Q.17 Name the branches of the internal thoracic artery.
Q.18 What type of movement of ribs take place during the respiration?
The anterior end of the ribs can move up during inspiration and down during expiration by rotation at costovertebral and costotransverse joints. This increases the anteroposterior diameter of the thorax.
Angular movement at manubriosternal joint of the upper six ribs leads to the forward movement of ribs.
In inspiration, the middle of the rib is raised. This occurs at the costotransverse and sternocostal joint at 7th to 10th ribs and increases the transverse diameter of the thorax.
Elevation of ribs is produced by external intercostal and depression by internal intercostal during quiet breathing.
Also read: Anatomy Question Collection
Also read: Anatomy Questions & Answers
Also read: Anatomy notes
Comments (0)