Inguinal Canal (Viva)
6 years ago 4926
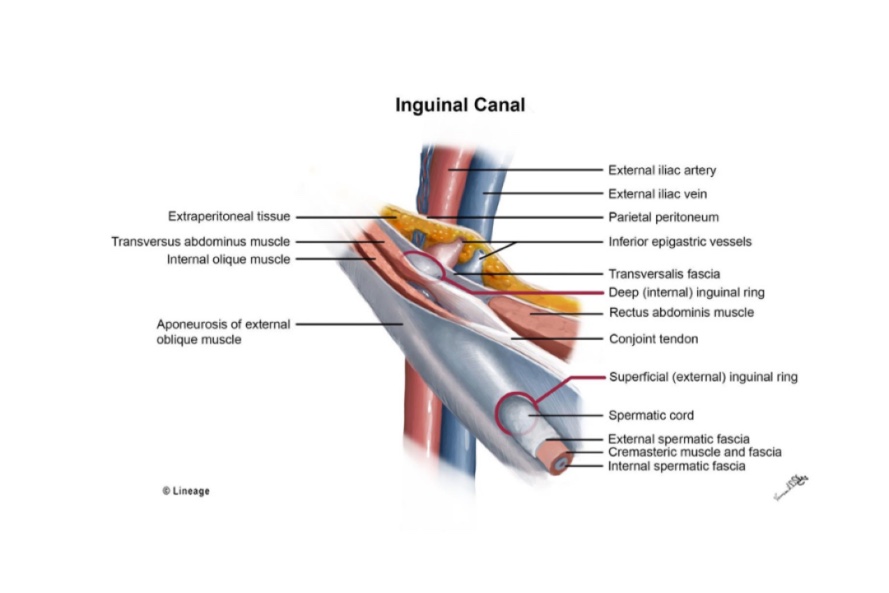
INGUINAL CANAL
Q.1 What is the position of the inguinal canal?
In the lower part of the anterior abdominal wall, just above the medial half of inguinal ligament. It extends from deep to superficial inguinal ring, downwards and medially.
Q.2 What is the surface marking of the deep inguinal ring?
Q.3 What is the surface marking of superficial inguinal ring?
Q.4 What are the boundaries of the inguinal canal?
Anterior
Posterior
Roof
Floor
Q.5 Name the structures passing through the inguinal canal.
Q.6 Name the structures passing through the deep inguinal ring.
Same as above except ilioinguinal nerve, which enters between external and internal oblique muscles and passes out through superficial inguinal ring.
Q.7 What are the boundaries of Hasselbach’s triangle?
Laterally: Inferior epigastric artery.
Medially: Lateral border of rectus abdominis.
Inferiorly: Medial half of inguinal ligament.
It is divided into two unequal portions by the obliterated umbilical artery.
Q.8 What is a hernia?
It is the protrusion of the contents of the abdomen (usually gut) through an opening or weak area in the wall of the body, e.g. femoral canal, inguinal canal, epiploic foramen.
Q.9 What are the factors which prevent the herniation through the inguinal canal?
Q.10 What are the different types of inguinal hernia?
Two types:
– Medial direct hernia: Medial to obliterated umbilical artery.
– Lateral direct hernia: Lateral to obliterated umbilical artery.
Q.11 What is incomplete and complete inguinal hernia?
Inguinal hernia is incomplete when it does not pass beyond the superficial inguinal ring. In complete hernia, the herniated gut descends in front of testis into tunica vaginalis.
Q.12 What are the main differences, between direct and indirect inguinal hernia?
| Direct inguinal hernia | Indirect inguinal hernia |
| Less frequent | More frequent |
| Placed over the body of the pubic bone. | Placed in the course of the inguinal canal. |
| Neck of the sac: Medial to the inferior epigastric artery |
Neck of the sac: Lateral to the inferior epigastric artery |
| Spermatic cord: Lies on its posterior |
Spermatic cord: Lies behind it and lateral sides. |
| Usually acquired. | Usually congenital. |
Q.13 How will you clinically distinguish an inguinal hernia from a femoral hernia?
An inguinal hernia lies above and medial to the medial end of the inguinal ligament at its attachment to the pubic tubercle. Femoral hernia lies below and lateral to the pubic tubercle.
Q.14 In which sex:
• Inguinal hernia common.
• Femoral hernia common and why?
Q.15 What can be the contents of a hernial sac?
Q.16.1 What is Littre’s hernia?
When the Meckel’s diverticulum present in the hernial sac.
Q.16.2 What is a ‘strangulated hernia’?
When the blood supply to hernial contents becomes impaired thus leading to the death of the tissue.
Q.17 How will you clinically distinguish a direct from an indirect inguinal hernia?
By deep ring occlusion test in cases of reducible hernia. The hernia is first reduced and deep (internal) inguinal ring is occluded with a fingertip and the patient is asked to cough while standing.
If it is an indirect hernia, as the deep ring is occluded, it prevents hernial contents from descending into scrotum. But a direct hernia will protrude as contents herniate through the posterior wall of the inguinal canal.
Q.18 What are the coverings of inguinal hernia?
Indirect hernia: From without inwards:
Direct hernia:
Q.19 What is the developmental origin of the Inguinal canal?
It represents the passage of gubernaculum through the abdominal wall. It extends from the caudal end of developing gonad to labioscrotal swelling.
Comments (0)