PR interval
3 years ago 4189
The PR interval is the period from the beginning of the P wave to the onset of the QRS complex. It represents the atrioventricular conduction time i.e. time taken for the cardiac impulse/ SA nodal impulse to spread over the atrium to the AV node & down the bundle of His.
PR interval consists of P waves and a PR segment (an isoelectric line). P waves indicate atrial depolarization. PR segment is the flat isoelectric line from the end of P waves to the onset of QRS complexes. PR segment represents the AV nodal delay to allow adequate ventricular filling.
The normal duration of P waves is less than 0.1 seconds (2.5 mm width in ECG paper).
Note:
| If you already know the basis of ECG and PR interval, we can directly head to the bottom of the page, where there is the algorithm for PR interval interpretation. |
Normal Duration of PR interval:
The normal duration of the PR interval is 120 ms - 200 ms i.e. 0.12 seconds - 0.2 seconds. The normal range of PR interval is 3 - 5 small boxes in the ECG graph i.e. up to 1 large box.
How to measure PR interval
For the measurement of the PR interval, think of P waves & PR segment. PR interval starts from the onset of P waves to the beginning of the QRS complex. The normal Duration of the PR interval is 120 - 200 milliseconds i.e. 0.12 - 0.2 seconds. This time interval corresponds to 3 - 5 small boxes in ECG paper.
To know the relationship between time & width/box in ECG paper
| 1 small box equals 1 mm. |
| 1 small box equals 40 ms (0.04 sec). |
| 3 small boxes equal to 3 mm. |
| 3 small boxes equal 120 ms (0.12 sec) (3 x 40 ms). |
| 1 large box contains 5 small boxes. |
| 1 large box equals 5 mm. |
| 1 large box equals 200 ms (0.2 sec) (5 x 40 ms). |
Prolonged PR interval:
If the PR interval is more than 200 ms (> 1 large box) is termed a prolonged PR interval.
A prolonged PR interval (over 200 ms) indicates slow conduction of cardiac impulse between atria and ventricle, usually due to slow conduction of cardiac impulse through the AV node.
The prolonged PR interval may be associated with AV node fibrosis, a high vagal tone that decreases cardiac activity, and medication that slows the AV node conduction i.e. beta blocker, hypokalemia, acute rheumatic fever.
Causes of prolonged PR interval:
The causes of prolonged PR intervals are
If the PR interval is more than 200 ms (> 1 large box) & constant, it indicates First-degree heart block.
In Second Degree Heart block, there is a progressive lengthening of PR interval with each successive beat, until one QRS complex is dropped/missed/absent. The P wave is not followed by the QRS complex.
In an Ectopic atrial rhythm, the P wave is inverted and the PR interval is prolonged (> 120 ms).
Short PR interval:
If the PR interval is less than 120 ms (< 3 small boxes) is termed a Short PR interval.
If the PR interval is less than 120 ms (< 3 small box), it indicates Pre-excitation syndrome. Lown-Ganong-Levine (LGL) syndrome & Wolf-Parkinson-White (WPW) syndrome are the two Pre-excitation syndrome.
Causes of PR interval:
Causes of Short PR interval are Pre-excitation syndrome i.e. LGL syndrome & Wolf Parkinson White Syndrome and Junctional Rhythm (AV nodal Rhythm). But for Junctional Rhythm, P waves should be inverted.
Junctional rhythm means cardiac impulses originate from the AV node. In ECG of Junctional Rhythm, the PR interval is short & P waves are inverted, or sometimes P waves absent also.
Pre-excitation syndrome
Pre-excitation syndrome means that there is an accessory pathway of cardiac impulse between the atria & ventricle. Lown-Ganong-Levine (LGL) syndrome & Wolf-Parkinson-White (WPW) syndrome are the two Pre-excitation syndrome.
How to differentiate Wolf Parkinson White (WPW) syndrome and Lown Ganong Levine (LGL) syndrome?
In Wolf Parkinson White (WPW) syndrome, there are the following ECG findings.
If dominant R waves are present in V1, it is Type A WPW syndrome. It indicates the left-sided accessory pathway of cardiac impulse.
If dominant S waves are present in V1, it is Type B WPW syndrome. It indicates the right-sided accessory pathway of cardiac impulse.
In Lown Ganong Levine (LGL) syndrome, there are the following ECG findings.
Variable PR interval
Variable PR intervals may represent different types of Heart blocks.
In Second Degree Heart block, there is a progressive lengthening of PR interval with each successive beat, until one QRS complex is dropped/missed/absent. The P wave is not followed by the QRS complex.
In Third degree Heart Block, there is variation in PR interval. There is no correlation between P waves & QRS complex as atria & ventricles are both contracting independently of each other. But P to P interval is regular and R to R interval is regular.
PR segment depression
PR segment depression may be present in pericarditis.
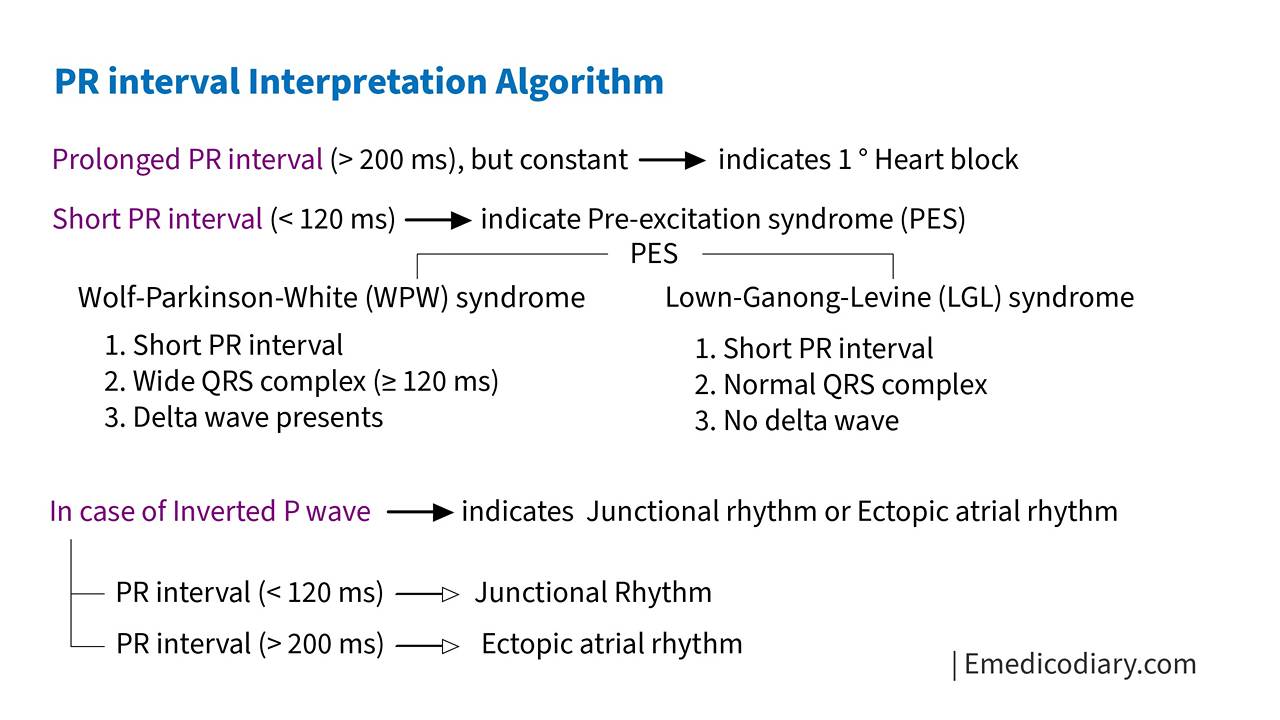
Algorithm for interpretation of PR interval
Diagnosing abnormalities through the interpretation of PR interval only is not possible. We have to look at both P waves & QRS complex along with the PR interval side by side. Here, in this algorithm of PR interval interpretation, we only focused on the important aspect in a straightforward way.
Prolonged PR interval (> 200 ms) but constant, indicates First degree Heart Block.
Short PR interval (less than 120 ms), indicates Pre-excitation syndrome i.e. Lown-Ganong-Levine (LGL) syndrome & Wolf-Parkinson-White (WPW) syndrome. Short PR interval in Ecg is usually presented as P waves immediately followed by QRS complex.
In Wolf Parkinson White (WPW) syndrome, there are the following ECG findings.
In Lown Ganong Levine (LGL) syndrome, there are the following ECG findings.
In the case of inverted P waves, except in aVR & V1 leads, it indicates Junction Rhythm or Ectopic atrial rhythm.
If a short PR interval (less than 120 ms), it indicates a Junctional rhythm. Junctional rhythm means cardiac impulses originate in the AV junction.
If prolonged PR interval (over 200 ms), it indicates Ectopic atrial rhythm. Ectopic atrial rhythm means cardiac impulse origin within the atria.

Comments (0)