Why Diabetics Must Never Ignore Foot Pain
2 months ago 183
Diabetes affects more than 537 million adults worldwide, and one of its most serious yet overlooked complications involves the feet. Every 30 seconds, a lower limb is lost to diabetes somewhere in the world. Despite this, millions of diabetic patients continue to dismiss foot pain, tingling, or sores as minor inconveniences that will resolve on their own.
In my clinical experience as a podiatrist, I have seen this pattern far too many times. A patient walks in with what started as a small blister or a mild aching sensation weeks earlier. By the time they sit in my examination chair, the wound has become infected, the tissue is breaking down, and in the most serious cases, the foot can no longer be saved.
This article explains exactly why diabetics must take foot pain seriously, what happens when they do not, and what steps to take to protect long-term mobility and health.
To understand why foot pain in diabetics demands immediate attention, it is important to first understand how diabetes affects the feet over time. Two key processes are responsible for most diabetic foot complications.
Persistently elevated blood sugar gradually damages the peripheral nerves, particularly those supplying the feet and lower legs. This damage, known as diabetic peripheral neuropathy, disrupts the normal ability to feel pain, heat, cold, and pressure.
The result is that patients lose their body's natural early warning system. A cut from an ill-fitting shoe, a blister from prolonged walking, or a small wound from walking barefoot can go entirely unnoticed. Without the signal of pain, the injury continues to worsen without any intervention.
Diabetes causes blood vessels to narrow and harden over time, a condition known as peripheral arterial disease (PAD). Reduced blood flow to the feet means that even a small cut or sore heals far more slowly than it would in a non-diabetic person. The immune system's ability to fight infection is also significantly impaired, making diabetic wounds highly prone to serious bacterial infection.
Together, these two conditions create a uniquely dangerous environment in the feet where injuries go unfelt, infections develop quickly, and healing is severely compromised.
Understanding how clinical findings are assessed is important in diabetic care. Medical professionals use standardised notation such as WNL (Within Normal Limits) to document normal examination results during routine diabetic foot assessments.
Many diabetic patients wait until pain becomes unbearable before seeking medical advice. However, because neuropathy often reduces sensation, pain may not even be present. The following warning signs should prompt immediate evaluation by a foot specialist, even if there is no significant pain.
If any of these signs are present, do not wait. Early evaluation is the single most important factor in preventing serious complications.
When diabetic foot problems are left untreated, they follow a predictable and often devastating progression. Understanding this pathway underscores why early action is so critical.
According to the International Diabetes Federation, diabetes accounts for approximately 60 percent of all non-traumatic lower limb amputations globally. Research consistently shows that around 15 percent of diabetic patients will develop a foot ulcer during their lifetime.
However, the same research confirms that with early specialist intervention, the risk of amputation can be reduced by up to 85 percent. This is a figure that every diabetic patient should know.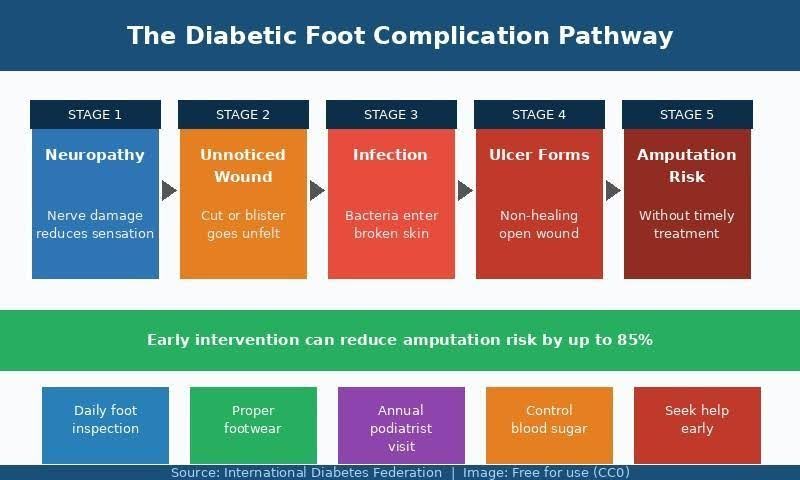
Certain foot conditions occur with significantly higher frequency in people living with diabetes. Recognising these conditions early allows for prompt treatment before they escalate.
Diabetic foot ulcers: Open sores that typically develop on the bottom of the foot over pressure points. They are the most common cause of diabetes-related hospitalisation and require immediate medical treatment.
Ingrown toenails: A seemingly minor condition that carries a disproportionately high infection risk in diabetic patients. Even a small breach in the skin around the nail can lead to serious infection rapidly.
Toenail fungus (onychomycosis): More prevalent in diabetic patients due to immune system changes. Fungal nails thicken over time, pressing into surrounding tissue and creating additional entry points for bacteria.
Calluses and corns: Develop over pressure areas and can break down the underlying skin if untreated, creating hidden wounds that may not be felt due to neuropathy.
Charcot foot: A serious condition where neuropathy leads to bone fractures and joint dislocations that go unnoticed, progressively causing deformity and collapse of the foot architecture.
Peripheral arterial disease (PAD): Reduced blood flow to the lower limbs that significantly slows wound healing and increases infection risk in any foot injury.
Many diabetic patients either delay seeking professional help or avoid it altogether out of concern about what they might be told. However, early evaluation consistently leads to better outcomes. You should seek professional assessment without delay if you notice any of the following.
For diabetic patients seeking specialist evaluation, the team at Beaver Valley Foot Clinic's diabetic foot care provides comprehensive assessments covering nerve sensitivity, circulation status, skin integrity, wound evaluation, and footwear recommendations. Early assessment at a dedicated diabetic foot clinic is one of the most effective steps a diabetic patient can take to protect long-term foot health.
Prevention plays a central role in diabetic foot care. The following daily habits are the same recommendations given to every diabetic patient in a clinical setting and have strong evidence behind them for reducing complication rates.
Alongside foot care, avoiding harmful habits is equally important for diabetic health management. The impact of lifestyle choices on circulatory and nerve health is significant, as explored in related health discussions on this site such as the health impacts of vaping and nicotine products, which highlights how nicotine constricts blood vessels and further impairs circulation in the lower limbs.
No amount of topical wound care or specialist treatment can fully compensate for poorly controlled blood glucose. Elevated blood sugar directly impairs the two mechanisms most critical to diabetic foot health: nerve function and blood circulation.
Working with a diabetes care team to maintain HbA1c levels within a target range, following a structured diet, staying physically active, and taking prescribed medications consistently all reduce the rate at which neuropathy and vascular damage progress. Good glycaemic control does not reverse existing nerve damage, but it significantly slows its worsening and gives wounds a substantially better environment to heal.
Comments (0)